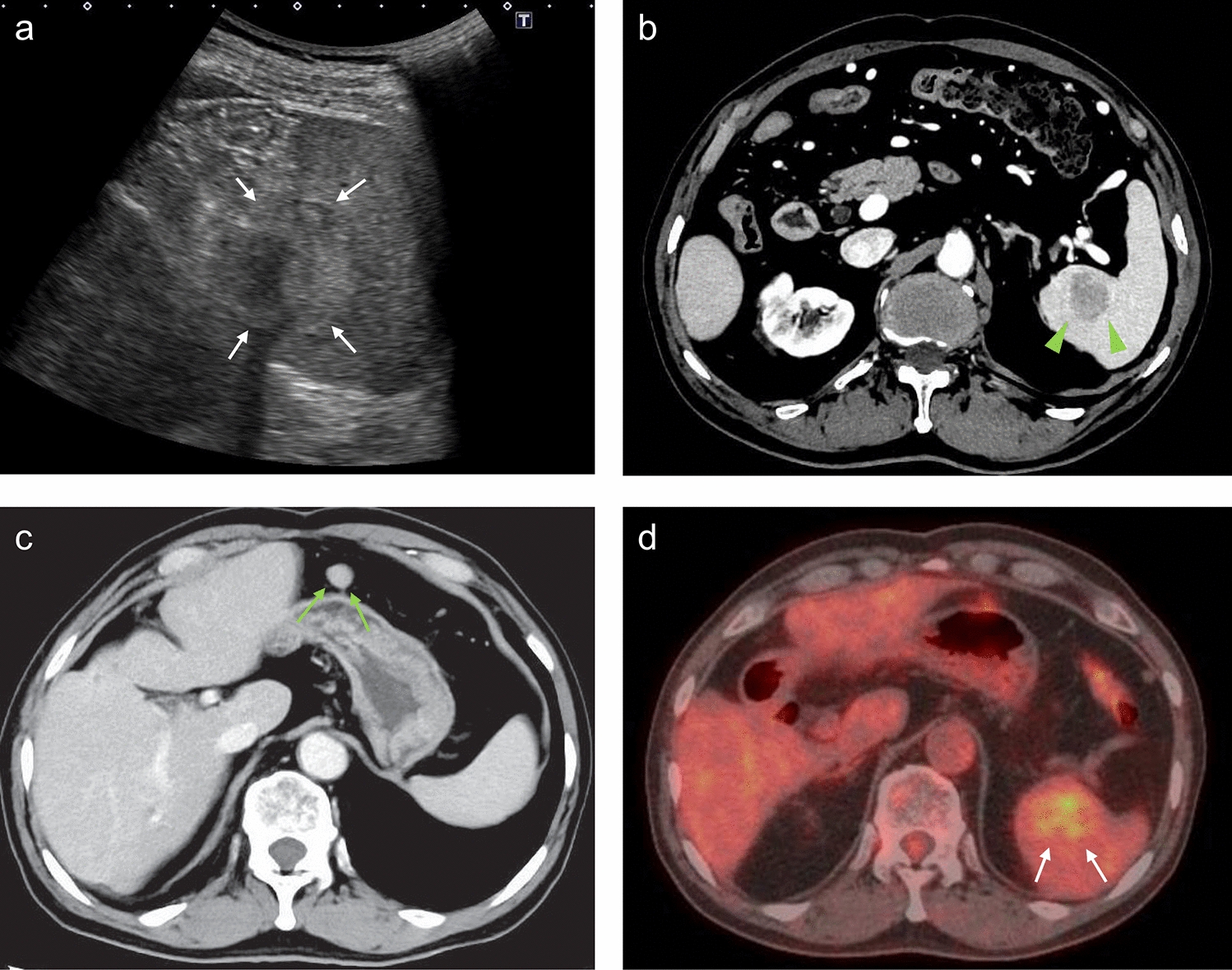
Various benign and malignant splenic lesions may spontaneously rupture. A previous report classified atraumatic splenic ruptures into six etiological groups, and neoplastic disorders were noted in 30.3% of the patients [8]. In the present case, the patient had a history of MALT lymphoma and HCC, which made accurately diagnosing the splenic lesion difficult. Because the concentrations of the tumor markers AFP and PIVKA-II increased gradually and ultrasound and CT scans showed that the tumor was seemingly buried in the spleen, we suspected splenic metastasis of HCC before the operation. However, based on the histopathological findings, the ruptured lesion was diagnosed as a splenic hilar LN metastasis.
The present case is unique in that spontaneous rupture occurred in a splenic hilar LN metastasis from HCC. Metastasis to a splenic hilar LN is generally uncommon in HCC, although metastasis to a perigastric LN has been previously reported, with an incidence of 10.8% [9]. In the present case, No. 4sb metastasis of HCC was observed. This finding suggests that HCC may have metastasized first to No. 4sb and then to the splenic hilar LN through lymphogenous spread. In addition, the mechanisms underlying LN metastatic rupture in HCC remain poorly understood. In a previous case, which was the first reported case of abdominal LN metastatic rupture from HCC, the HCC tissue in the LN appeared to cause a breakdown of the capsule either by increased pressure or by direct HCC invasion [7]. In the present case, the metastatic splenic hilar LN enlarged rapidly within 2 months from diagnosis to spontaneous rupture. A few normal LN structures remained in the splenic hilar LN, and the LN was filled with poorly differentiated HCC tissue. Thus, HCC tissue under the LN capsule may have increased intratumoral pressure, leading to spontaneous rupture.
Rupture of LN metastasis in HCC is extremely rare, and to the best of our knowledge, only four cases, including our case, have been reported to date (Table 2) [5,6,7]. All patients were male, and their ages ranged from 55 to 79 years. Notably, our patient was older than any of the previous patients. The location of LN metastasis was the mediastinal LN in two patients, the peripancreatic LN in one, and the splenic hilar LN in our case. Two patients underwent transcatheter arterial embolization (TAE). Our patient is the only reported patient to have undergone surgical resection. The remaining patient received conservative treatment and LN metastasis rupture was revealed by autopsy. Surgical resection and TAE are considered optimal treatments for ruptured HCC. For most patients with ruptured HCC, TAE followed by surgical resection is the preferred first-line treatment option, except for those with poor liver function and advanced tumors [10]. However, the optimal treatment strategy for ruptured LN metastases from HCC remains unclear because little data are available. Based on the findings in Table 2, it is remarkable that our patient survived for at least 25 months after LN metastatic rupture, as the other three reported patients died within 4 months. Thus, our case suggests that surgical resection for LN metastatic rupture may lead to a favorable survival outcome compared to TAE alone, if curative resection is possible.
Table 2 The reported cases with spontaneous rupture of lymph node metastasis of HCCOne possible reason for the relatively long-term survival in this case was the low burden of intrahepatic tumors. In general, the prognosis of patients with HCC and LN metastasis is poorer than that of patients without LN metastasis [11]. However, previous literature has shown that the intrahepatic tumor status predicts the prognosis of HCC patients with extrahepatic metastasis [12, 13], and it has been reported that optimal management of intrahepatic lesions and complete removal of the LN metastasis may improve the survival outcomes in HCC patients with LN metastasis [14, 15]. Moreover, some researchers have reported that surgical resection of extrahepatic metastases, such as adrenal gland and peritoneal metastases, results in long-term survival [16, 17]. In the present case, the intrahepatic lesion was well controlled by past liver resection, and the ruptured metastatic splenic hilar LN and swollen No. 4sb LN were the only HCC metastatic lesions and resectable lesions as well. Therefore, a surgical resection was performed. Another possible reason is that the recurrences of HCC after splenectomy were well controlled with liver resection and atezolizumab plus bevacizumab. Our findings suggest that spontaneous rupture may occur in metastatic LN of HCC, and patients with LN metastasis should receive close surveillance and appropriate management to improve survival.
In conclusion, we encountered an extremely rare case of spontaneous rupture of a splenic hilar LN metastasis from HCC that required emergency splenectomy. Although this life-threatening complication may occur in cases of LN metastasis from HCC, emergency surgery is one of the effective treatment options that can lead to hemostasis and favorable survival.




留言 (0)