Post-embolization syndrome-like symptoms due to shedding of necrotic material of hepatocellular carcinoma into the bile duct following transcatheter arterial chemoembolization: an instructive case
We consider that in the present case, fragments of a necrotic tumor became detached from the bile duct wall after TACE and migrated into the common bile duct, causing obstructive jaundice. Migration of intraductal-tumor invasion in hepatocellular carcinoma after TACE is very rare [5,6,7], but has been noted to occur more often than might have been reported [8]. It has also been reported that some patients remain asymptomatic even when necrotic tissue drains into the bile duct [8]. In patients with hepatocellular carcinoma, who are more likely to have reduced hepatic reserve, there is a risk of liver failure due to worsening liver function. Therefore, if fever, abdominal pain, or liver dysfunction persist or if new symptoms are observed after several days, it is advisable to perform appropriate imaging studies and closely examine the patient for other causes, rather than simply attempting to reduce the fever. In addition, as excretory tumor tissue is difficult to detect by plain CT in the absence of iodine oil accumulation, some such cases may have been missed after being judged as postembolic syndrome due to TACE, and no appropriate treatment given [9]. From this perspective, the present case is very instructive. We believe it is very important to raise awareness of the existence of such cases. Endoscopic ultrasound (EUS) has a much higher detection rate of common bile duct stones than other imaging tests and is a very useful test for identifying structures in the bile duct [10]. EUS is also a low-risk test and should be considered in patients with no specific abnormalities on CT scan.
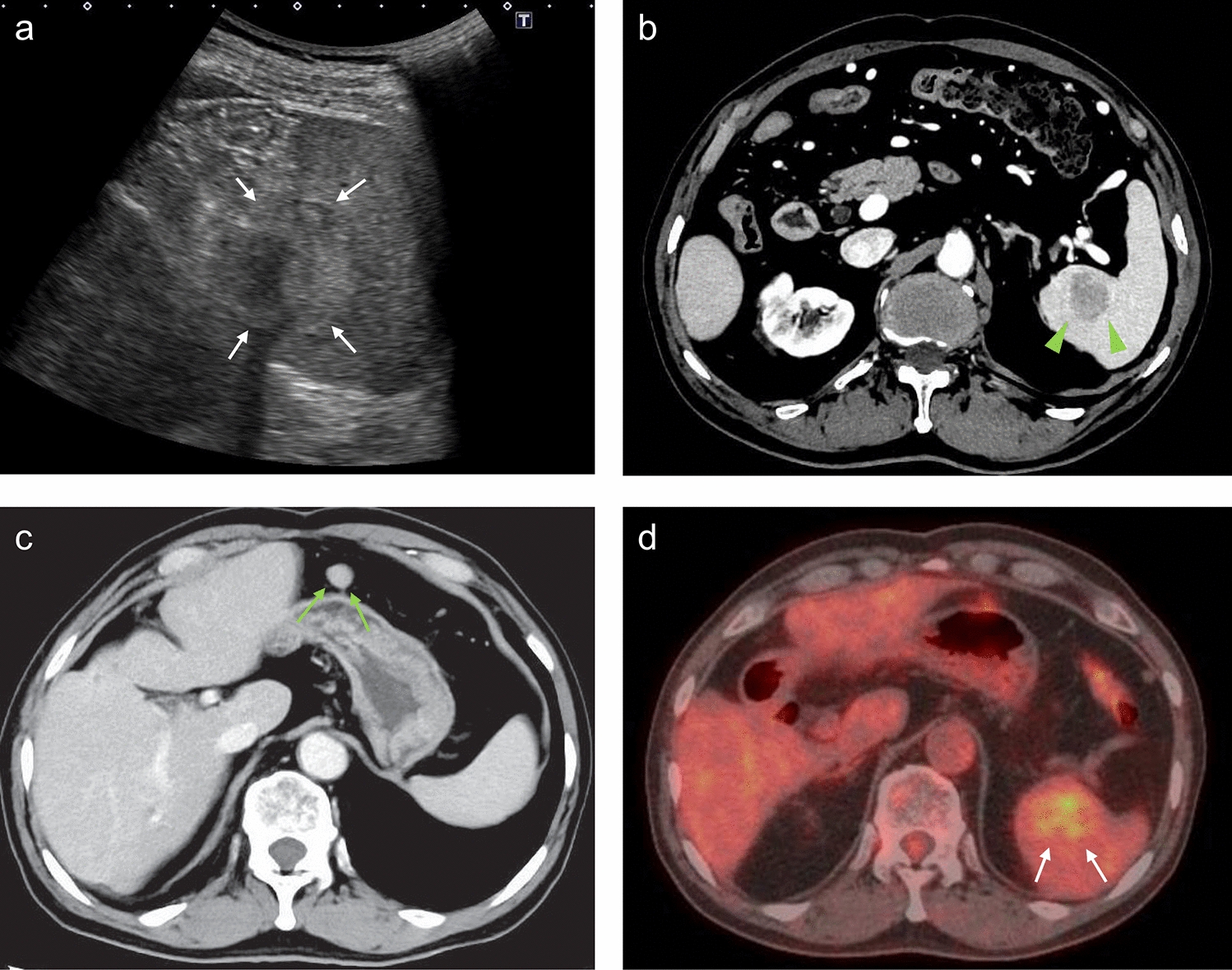
A previous study has reported that necrotic tissue can easily be misidentified as bile duct stones because of the accumulation of highly absorbable iodine oil in the generally desquamated tumor necrotic tissue [9]. In the present case, we suspected bile duct stones on CT, but as the HCC was originally suspected to have infiltrated the intrahepatic bile duct, a definitive diagnosis was obtained after submitting the removed specimen for pathologic examination. It is important to confirm the preliminary imaging studies thoroughly and to recognize that patients with suspected bile duct invasion of HCC are particularly prone to developing obstructive jaundice due to tumor necrosis [7]. Other factors reported to be associated with obstructive jaundice due to the shedding of necrotic tumor into the bile duct include the total number of TACE procedures, the presence of bile duct dilation on CT, and tumor location [7]. However, it should be noted that TACE causes marked ischemic necrosis not only in the vascular bed of the tumor but also in the adjacent bile ducts, which can occur even in patients without bile duct invasion [9, 11]. It has been reported that in patients with an HCC greater than 5 cm in size that is in contact with the left and right hepatic ducts, even without bile duct invasion, it is not uncommon for necrotic tumors to be excreted into the biliary system after TACE [9]. It has been reported that the mechanism by which necrotic tumors are excreted into the biliary system, even in tumors without intraductal-bile duct invasion, is that bile ducts near the tumor are mainly supplied only by arterial blood, and that damage caused by TACE may result in fistula formation between necrotic tumor and the biliary system. It is important to be fully aware of the possibility of obstructive jaundice and biliary tract infection due to the shedding of necrotic tumor into the bile duct after TACE. In addition, a variety of anticancer drugs have been launched in recent years; therefore, and not only TACE but also other anticancer drugs may cause obstructive jaundice due to similar tumor necrosis, which requires caution.




留言 (0)