
記住我

There is a staggering global burden of intimate partner violence (IPV)—defined as emotionally, sexually, and physically abusive or manipulative behaviors inflicted by a romantic partner.1 The World Health Organization2 provides lifetime IPV prevalence estimates of 26% worldwide and 45% in Uganda for women aged 15 and older. The most recent Demographic Health Survey in Uganda indicates that 39% of ever-married women and men had reported emotional, sexual, or physical IPV during the past year.3 IPV has implications for increased risk of HIV acquisition and reduced health outcomes for people living with HIV.4–6 Prospective studies in South Africa and Uganda indicate that HIV incidence is as much as 50% higher among women with a history of IPV compared with their IPV-unexposed counterparts.7,8 For individuals in serodifferent partnerships, IPV may arise after disclosure of a positive HIV status due to fears surrounding onward transmission to the negative partner, lack of trust, and/or concerns about sexual unfaithfulness being the possible source of HIV infection.9 People living with HIV may be more likely to report experiences of IPV as a result of behavioral changes related to their HIV diagnosis including going to collect and, subsequently, taking HIV medication as well as attempting to engage one's partner in discourse about HIV testing and/or prevention options.4,5,10,11 There are well established associations between IPV exposure and poor mental health outcomes including post-traumatic stress disorder, depression, and substance use12,13 which may highlight key mechanisms through which IPV may exert its influence on HIV treatment and prevention outcomes.
HIV pre-exposure prophylaxis (PrEP) and antiretroviral treatment (ART) use prevent the onward sexual acquisition or transmission of HIV.14,15 The use of these biomedical tools may be especially pertinent for reducing HIV transmission risk among partners newly aware of their serodifferent status and for whom violence may be a defining relationship feature. However, current regimens require high levels of compliance with daily pill-taking to confer HIV protection and experiences of IPV may undermine the consistent and cooperative use of ART and PrEP in a relationship. There is evidence documenting the detrimental influence of IPV on ART adherence16,17; however, reports of an association between IPV and PrEP use are more ambiguous—with some findings indicating that IPV exposure may encourage PrEP use18,19 and others suggesting that it may discourage PrEP use.20,21 Furthermore, although IPV is definitionally interpersonal, the existing evidence base outlining the association between IPV exposure and HIV-related outcomes predominately focuses on individual level factors.
Because PrEP and ART use in serodifferent couples may be highly dependent on partner cooperation, it is of interest to contextualize the association between IPV exposure and PrEP/ART adherence by evaluating perspectives of both partners. Expanding the available evidence base to feature a more dynamic conceptualization of IPV and HIV may enhance our capacity to identify and subsequently intervene on these interconnected experiences using concurrent and couples-based strategies, thereby improving health outcomes for both conditions. We assessed individual and relationship factors in our evaluation of the association between IPV and PrEP/ART adherence among both members of serodifferent couples in Uganda.
METHODS Participants and ProceduresWe conducted a secondary analysis of the Partners PrEP Program (ct.gov #NCT03586128) data set.22 This implementation study was a stepped-wedge cluster randomized trial that evaluated integrated PrEP and ART delivery to HIV-negative members of HIV serodifferent couples accessing care in 12 ART clinics located in the Wakiso and Kampala districts of Uganda. From June 2018 through December 2020, heterosexual HIV serodifferent couples from the trial were offered enrollment into a research component. The present analysis features data from participants enrolled to this add-on research component. Eligibility criteria for couples enrolling into this add-on research component of the study were being in an HIV serodifferent partnership; having mutually disclosed HIV status; aged 18 years and older; able to provide informed consent; sexually active with one another and willing to attend clinical visits together. For the HIV-positive partner, additional eligibility criteria included having received a recent HIV diagnosis in an HIV serodifferent couple. For the HIV-negative partner, additional eligibility criteria included not being a PrEP user at the time of enrollment and being eligible for PrEP according to World Health Organization or Ugandan national guidelines.
The research component involved more detailed procedures intended to enhance understanding of behaviors related to PrEP and ART use. Specifically, participants enrolled in the research component attended quarterly visits (for up to 24 months after enrollment) at the research clinic for assessments of demographics, behavioral characteristics (eg, alcohol and drug use; sexual practices), experiences of violence and biological sample collection for objective adherence measurements (ie, viral load blood testing for partners living with HIV and tenofovir-diphosphate (TFV-DP) testing of dried blood spots for HIV-negative partners). During study visits, trained clinical research staff administered questionnaires in the participant's preferred language (ie, Luganda or English) in a private location. Participant behavioral characteristics included problematic alcohol use which was assessed using the Rapid Alcohol Problems Screen23 and defined when the respondent indicated that, in the prior month, they had (1) felt guilt or remorse after drinking; (2) been told by friend or a family member of things that they had done while drinking and which they could not remember; (3) failed to do what was normally expected of them due to their drinking; or (4) sometimes drank alcohol on waking. Data about participant sexually transmitted infections were derived from abstracting participant medical information about syndromic sexually transmitted infections from health facility charts.
OutcomeThe primary outcomes for this analysis were low adherence to ART among partners living with HIV and low adherence to PrEP among partners without HIV. Both measures were evaluated at 1 month after enrollment and at all subsequent quarterly follow-up visits (up to 24 months) using self-report or biological measures. In instances in which self-report and objective adherence results were discrepant, we relied on the objective adherence results (eg, viral load, TFV-DP quantity). For ART users, low adherence was defined as having a detectable HIV viral load (ie, ≥50 copies/mL) at the time of sample collection or using one or more self-report measures: if ART use in the past month was “Very poor,” “Poor,” or “Fair”; if they took ART “Not at all” or “Some days”; or if they had failed to take ART ≥7 days (vs. <7 days) in the past month. If none of these measures indicated low adherence, ART users were classified as having good adherence. For HIV-negative partners, we randomly selected 10% of participants for dried blood spot testing at quarterly visits subsequent to visits when PrEP was dispensed. Samples were tested for TFV-DP by liquid chromatography tandem mass spectrometry at the University of Colorado,24–26 and low adherence was defined as having TFV-DP <31.25 fmol/punch.27 In addition, low PrEP adherence was defined by self-report measures: PrEP use in the past month was “Very poor,” “Poor,” or “Fair”; they took PrEP “Not at all” or “Some days.” Time points without any indication of low adherence were classified as having good adherence.
Exposure to IPVExposure to physical or sexual IPV was assessed quarterly using a modified version of the Conflict Tactics Scale.28 This instrument has been applied in diverse settings, including in Uganda.29,30 At the enrollment visit, participants were asked about physical or sexual IPV history from any sexual partner in the past 1 year; at subsequent follow-up visits, participants were asked about physical or sexual IPV exposure in the past 1 month. Research staff provided examples of physical (eg, slapped, kicked, choked, pushed, and burned) or sexual (eg, forced you to have sex by hurting you or holding you down) violence in a manner that was considered culturally appropriate. Sexual or physical IPV exposure was indicated if the participant reporting affirmatively to any of the posed queries. If participants indicated that they were experiencing violence during the interview, they were subsequently connected to facility staff for further screening, referral, and/or management of IPV.
We assessed perceived powerlessness in sexual partnerships as a secondary predictor, using the relationship control subscale of the Sexual Relationship Power Scale (SRPS) to measure this variable.31 This validated survey instrument has been extensively leveraged to assess perceptions of power inequities within sexual relationships—specifically inquiring about relationship control and decision-making dominance.32–34 The SRPS relationship control subscale consists of statements such as, “I feel trapped in our relationship”; “My partner gets more out of our relationship than I do”; and “My partner always wants to know where I am.” Participants indicated their level of agreement using a 4-point Likert scale ranging from “Strongly disagree” to “Strongly agree.” Based on the distribution of participants' SRPS scores, we categorized scores into 1 of 3 groups—low, moderate, or high—based on tertiles of the SRPS score distribution. Higher SRPS scores were indicative of greater perceived powerlessness within the respondent's relationship. While questions assessing IPV exposure (ie, either physical or sexual) inquired about any recent sexual partner, SRPS statements were expressly framed in relation to the partner with whom the participant had enrolled in the research study.
Statistical AnalysisTo assess whether physical or sexual IPV is associated with low adherence, we estimated odds ratio (OR) through binomial generalized linear mixed-effects regression models incorporating a random effect to account for repeated measures within the same participants. Separately, among partners with HIV, we assessed associations with low adherence to ART, and among HIV-negative partners, we assessed associations with low adherence to PrEP. Secondarily, we assessed the association between SRPS and low adherence. In addition, we assessed the respondent's partner's IPV exposure or SRPS score on the participant's adherence. Unless otherwise stated, statistical models were adjusted for sex at birth, age, and condomless sex a priori given their known relationship with IPV and adherence. Analyses were conducted using R version 4.2.2.35
EthicsAll participants provided written informed consent in English or Luganda. The study protocol received ethical approval from the University of Washington Human Subjects Division (STUDY00000320), the Uganda National HIV/AIDS Research Committee (ARC 194), and the Uganda National Council for Science and Technology (HS 2381).
RESULTS Participant CharacteristicsWe enrolled and followed both partners in 149 heterosexual HIV-serodifferent couples from June 2018 to December 2021 (Table 1). Of these couples, 96 (64%) were couples in which the partner living with HIV was female. Most (80.5%) couples reported that they were married or cohabitating. The median age for participants living with HIV was 27 years (interquartile range: 23, 32) and 29 (25, 33) for HIV-negative participants. At enrollment, approximately 20% of participants living with HIV and 19% of HIV-negative participants reported having experienced sexual or physical violence in the past 1 year. Most participants reporting IPV indicated that it was physical in nature. The median SRPS score was 19 (16, 22) for participants living with HIV and 18 (15, 21) for their HIV-negative partners (with higher scores indicating greater perceptions of relationship powerlessness). Approximately 3% of participants living with HIV and 2% of HIV-negative partners reported a syndromic sexually transmitted infection at enrollment. Retention was high with 84% of expected ART follow-up visits and 86% of PrEP follow-up visits being attending. The median duration of follow-up for HIV-negative partners was 6 months (3, 9) and 6 months (3, 12) for partners living with HIV. By any measure (ie, self-report or biomarker data), we observed good adherence to ART in 95% of visits and PrEP in 64% of visits over the course of the follow-up period. For HIV-negative partners with data available from tenofovir testing and self-report adherence, 88.2% of observations were concordant. For partners living with HIV and data from viral load testing and self-report adherence, 84.6% of observations were concordant.
TABLE 1. - Enrollment Characteristics of 149 Couples Enrolled in the Partners PrEP Program Negative Partner (N = 149) Positive Partner (N = 149) Age in yr, median (IQR) 29 (25, 33) 27 (23, 32) Female sex at birth—no. (%) 53 (35.6) 96 (64.4% Marital status* Never married—no. (%) 5 (3.4) Married—no. (%) 99 (66.4) Living together—no. (%) 21 (14.1) Missing—no. (%) 24 (16.1) Sexually transmitted infections Syndromic STI—no. (%) 3 (2) 5 (3.4) Syphilis 0 (0) 2 (1.3) Other, unspecified 3 (2) 3 (2) Alcohol use in past 30 d Any alcohol use—no. (%) 36 (24.2) 32 (21.5) Problematic alcohol use—no. (%) 14 (9.4) 10 (6.7) Sexual behaviors in past 30 d Median number of sex acts with study partner, median (IQR) 5 (2, 10) 5 (2, 10) Any condomless sex act with study partner—no. (%) 100 (67.1) 99 (66.4) Any sex with another partner—no. (%) 17 (11.4) 11 (7.4) Any condomless sex act with another partner—no. (%) 15 (10.1) 11 (7.4) Any transactional sex—no. (%) 0 (0) 2 (1.3) Partner violence in past yr Slapped—no. (%) 21 (14.1) 23 (15.4) Kicked—no. (%) 18 (12.1) 19 (12.8) Forced to have sex—no. (%) 8 (5.4) 8 (5.4) Any reported violence—no. (%) 28 (18.8) 29 (19.5) Sexual relationship power score Median (IQR) 18 (15, 21) 19 (16, 22) Low (0–16) 53 (35.6%) 49 (32.9%) Moderate (17–20) 49 (32.9%) 49 (32.9%) High (21–33) 47 (31.5%) 51 (34.2%)*Marital status is based on data reported by partner living with HIV.
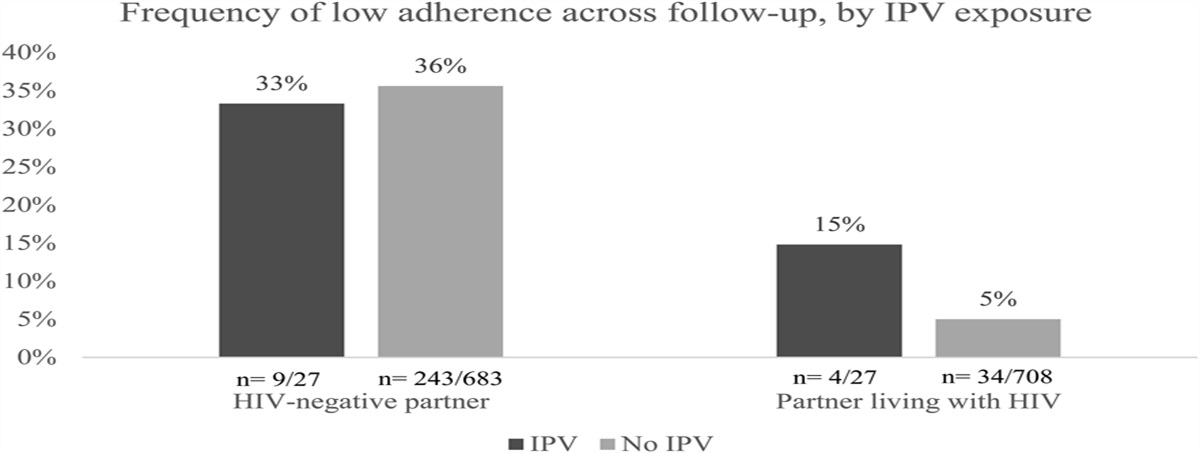
IPV was reported at 4% (29/732) of follow-up attended visits by HIV-negative partners and 4% (27/735) of follow-up visits attended by partners living with HIV. HIV-negative participants with recent IPV exposure had comparable odds of low PrEP adherence compared with those who had not reported recent IPV exposure [33% vs. 36%, OR = 0.84, 95% confidence interval (CI): 0.36 to 1.95, Fig. 1 and Table 2]. HIV-negative participants whose partners reported IPV exposure were less likely to have low PrEP adherence compared with those whose partners did not report IPV (OR = 0.36, 95% CI: 0.13 to 0.95). Partners living with HIV who reported recent IPV exposure were more likely to have low ART adherence (15% vs. 5%, OR = 4.78, 95% CI: 1.48 to 15.42, P = 0.009). For participants living with HIV, we observed no statistically significant association between their HIV-negative partner reporting exposure to IPV and ART adherence.
 FIGURE 1.:
FIGURE 1.: Participants reporting IPV (ie, physical or sexual) during follow-up.
TABLE 2. - Associations Between IPV (ie, Physical or Sexual) and Low Adherence to ART/PrEP Crude Adjusted* Adjusted† (With Partner IPV Exposure) OR (95% CI) P OR (95% CI) P OR (95% CI) P HIV-negative partner IPV 0.91 (0.40–2.05) 0.81 0.84 (0.36–1.95) 0.69 1.43 (0.54–3.74) 0.47 IPV (primary partner) 0.38 (0.14–1.02) 0.06 — — 0.36 (0.13–0.95) 0.05 Partner living with HIV IPV 3.08 (1.18–8.07) 0.02 4.78 (1.48–15.42) 0.01 3.84 (1.16–12.78) 0.03 IPV (primary partner) 2.34 (0.77–7.11) 0.14 — — 2.56 (0.85–7.64) 0.09Bolded entries emphasize P-values less than or equal to significance level of 0.05.
The adjusted column is blank for analyses in which the respondent's partner's IPV exposure is incorporated as predictor variable. Relevant findings are represented in far-right column.
*Adjusted for sex at birth, age, and report of any condomless sex.
†Adjusted for partner's report of IPV and sex at birth, age, and any condomless sex.
Median SRPS-Relationship Control subscale score was 18 (15, 21) for HIV-negative partners. Compared with those with low (ie, low perceived relationship powerlessness) scores on the Relationship Control SRPS subscale, HIV-negative participants with moderate perceived relationship powerlessness were less likely to have low PrEP adherence (OR = 0.57, 95% CI: 0.36 to 0.90, P = 0.015, Fig. 2 and Table 3). Compared with HIV-negative participants whose partners had low perceived relationship powerlessness, those whose partners had high perceived relationship powerlessness were less likely to have low PrEP adherence (OR = 0.56, 95% CI: 0.34 to 0.93, P = 0.025). For partners living with HIV, median SRPS-Relationship Control score was 19 (16, 22). We observed no statistically significant association between an individual's or their partner's perceptions of relationship powerlessness and ART adherence.
 FIGURE 2.:
FIGURE 2.: Participant SRPS category during follow-up.
TABLE 3. - Associations Between Sexual Relationship Power–Relationship Control Scale and Low Adherence to ART/PrEP Crude Adjusted* Adjusted† (With Partner IPV Exposure) OR (95% CI) P OR (95% CI) P OR (95% CI) P HIV-negative partner Low (0–16) Ref — Ref — Ref — Moderate (17–20) 0.61 (0.39–0.95) 0.03 0.57 (0.36–0.90) 0.02 0.61 (0.36–0.97) 0.04 High (21–33) 0.66 (0.40–1.07) 0.09 0.65 (0.40–1.08) 0.09 0.73 (0.44–0.90) 0.24 Low (0–16) [primary partner] Ref — — — Ref — Moderate (17–20)Bolded entries emphasize P-values less than or equal to significance level of 0.05.
The adjusted column is blank for analyses in which the respondent's partner's SRPS score is incorporated as predictor variable. Relevant findings are represented in far-right column.
*Adjusted for sex at birth, age, and report of any condomless sex.
†Adjusted for partner's score on SRPS-Relationship Control subscale, sex at birth, age, and any condomless sex.
In this secondary analysis leveraging data from a prospective study with heterosexual HIV-serodifferent couples in Uganda, we observed relatively high levels of PrEP and ART adherence, regardless of IPV exposure status or relationship power. Recent physical or sexual IPV was reported at approximately 4% of follow-up visits for HIV-negative partners and for partners living with HIV. In general, reports of recent exposure to either physical or sexual were less common over the course of the follow-up period. IPV exposure among participants living with HIV was associated with low ART adherence; however, we did not observe an association between ART adherence and the participant's partner reporting IPV exposure. Our findings align with prior studies assessing the relationship between IPV and ART, with consistent observations of an association between IPV exposure and lower adherence to ART.36,37
For HIV-negative participants, recent exposure to IPV was not associated with PrEP adherence; however, if the participant's partner reported recent IPV exposure, then low PrEP adherence was more likely. Diverse factors may contribute to the latter finding. HIV-negative individuals who use violence in their relationship may experience emotions such as guilt, shame, or worthlessness for causing harm to their partner. There is evidence to suggest that individuals struggling with low self-perception may be less likely to engage in self-care behaviors such as medication adherence.38,39 In addition, individuals who use violence against their romantic partner may not receive optimal emotional support from said partner (eg, reminders and encouragement to take medication). Indeed, there is evidence to suggest that individuals with weak emotional support networks, including lack of partner support, may struggle with medication adherence.40,41 Furthermore, compared with HIV-negative participants reporting low levels of relationship powerlessness, those who reported moderate powerlessness were more likely to be PrEP adherent. A possible explanation for this finding is that the HIV-negative partner, amidst a period of relational volatility (ie, after having learned of their partner's HIV positivity), may attempt to exert agency through PrEP taking and, potentially, through the use of violence against their partner living with HIV. Of note, all couples who participated in this research were married or in committed partnerships. Despite the challenges of learning of their serodifferent status, the nature of their union and their willingness to participate in research alongside their partner may be reflective of greater relational stability and/or acceptance of their serodifference compared with individuals in less committed unions. Thus, in our cohort, HIV-negative partners may have been sufficiently empowered and compelled to exert control through PrEP taking during an otherwise tumultuous period. Presently, there is no definitive consensus regarding the role of perceived relationship control on PrEP adherence. Emerging evidence offers mixed findings on the association, with some reports indicating better PrEP adherence when participants report greater perceived power in their relationship.42
An estimated 19% of negative partners and 20% of positive partners reported physical or sexual IPV within the past year at baseline. These findings are lower than recent population estimates in Uganda indicating that 29% of ever-married men and women reporting physical or sexual IPV in the past 1 year.3 Given that couples in this study had mutually disclosed their HIV status and had sufficient relationship stability to enroll in research procedures together, their experiences of violence and relationship characteristics may differ from the general population, limiting the generalizability of our findings. In addition, in contrast to reported IPV exposure at enrollment, reports of violence were less common during follow-up. This observation may have been due to inquiries of violence during follow-up being confined to a shorter duration (ie, the past month) compared with enrollment visits during which we assessed past-year violence. Further limitations include our reliance on self-reported data to assess adherence to PrEP and ART as well as other highly stigmatized relationship traits including IPV history and feelings of powerlessness. We attempted to address potential issues of response bias by leveraging research assistants who were of the same community and able to speak the same language as participants. In addition, we also supplemented self-reported adherence data with objective biomarker data to assess PrEP and ART use and provided context on the extent to which these data sources were in agreement. However, it is important to note that objective biomarker data were not always available for comparison against self-report data because of the cost of these laboratory analyses that necessitated selecting a subsample for analysis. Questionnaires were also administered in a private location in an effort to encourage participants to speak freely about their experiences and perceptions. Despite these safeguards, IPV and adherence data may have been underreported because of social desirability response bias. Furthermore, questions related to IPV were general in nature, and responses about sexual or physical violence may have referred to any sexual partner and not necessarily the partner with whom the participant had enrolled to research procedures. Another point for potential concern is that our analysis featured a relatively small number of follow-up visits during which IPV was observed. This limits statistical power and may have inhibited our ability to identify more moderate statistically significant relationships.
Understanding the ways in which violence manifests and influences adherence behaviors for individuals in serodifferent couples will support more targeted interventions that identify and interrupt experiences of violence for couples. In this study, 2 measures of relationship volatility—recent history of physical or sexual IPV and relationship powerlessness—demonstrated varied relationships with PrEP and ART adherence. Recent history of physical or sexual IPV was associated with low adherence to ART while perceptions of greater relationship powerlessness were associated with good PrEP adherence. In addition, when HIV-negative participants' partners reported greater relationship powerlessness, this was also associated with good PrEP adherence. Couples-based interventions that neutralize maladaptive behaviors in relationships—including the use of violent, manipulative, and/or controlling tactics—and encourage positive relational dynamics may support more cooperative use of PrEP/ART for individuals within serodifferent couples and, subsequently, improve health outcomes for both partners. Future research is needed to evaluate dynamic experiences of IPV while safely taking into consideration both individual—as well as relational influences on ART and PrEP adherence. The continued elaboration of this evidence base will support the identification and implementation of bespoke opportunities that target couples-based HIV and IPV prevention strategies.
ACKNOWLEDGMENTSThe authors thank the couples who participated in this project for their dedication and trust in the research staff and process.
APPENDIX. Partners PrEP Program Study TeamRenee Heffron (Protocol chair), Jared M. Baeten, Jane M. Simoni, Deborah Donnell, Ruanne Barnabas, Katherine K. Thomas, Dorothy Thomas, Erika Feutz, Cole Grabow, Allison Meisner, Kristin Ciccarelli, Caitlin Scoville, Katrina Ortblad [University of Washington (Seattle)], Andrew Mujugira, Timothy R. Muwonge, Joseph Kibuuka, Lylianne Nakabugo, Florence Nambi, Mai Nakitende, Diego Izizinga, Vicent Kasita, Brenda Kamusiime, Alisaati Nalumansi, Collins Twesige, Grace Kakoola, Charles Brown, Sylvia Namanda [Infectious Diseases Institute (Kampala, Uganda)], Herbert Kadama [Uganda Ministry of Health (Kampala, Uganda)], Norma C. Ware, Monique A. Wyatt, Emily Pisarski [Harvard University (Boston)], Ingrid T. Katz [Brigham & Women's Hospital (Boston)].
REFERENCES 1. World Health Organization. Responding to Intimate Partner Violence and Sexual Violence against Women: WHO Clinical and Policy Guidelines. Geneva, Switzerland: World Health Organization; 2013. 2. World Health Organization. Violence Against Women Prevalence Estimates, 2018: Global, Regional and National Prevalence Estimates for Intimate Partner Violence against Women and Global and Regional Prevalence Estimates for Non-partner Sexual Violence Against Women. Geneva, Switzerland: World Health Organization; 2021. 3. Uganda Bureau of Statistics (UBOS) and ICF International. Uganda Demographic and Health Survey 2016. Kampala, Uganda; Rockville, MD: UBOS and ICF; 2018. 4. Meskele M, Khuzwayo N, Taylor M. Intimate partner violence against women living with and without HIV, and the associated factors in Wolaita Zone, Southern Ethiopia: a comparative cross-sectional study. PLoS One. 2019;14:e0220919. 5. Osinde MO, Kaye DK, Kakaire O. Intimate partner violence among women with HIV infection in rural Uganda: critical implications for policy and practice. BMC Women's Health. 2011;11:50–57. 6. Ogbonnaya IN, Wanyenze RK, Reed E, et al. Prevalence of and risk factors for intimate partner violence in the first 6 months following HIV diagnosis among a population-based sample in rural Uganda. AIDS Behav. 2020;24:1252–1265. 7. Jewkes RK, Dunkle K, Nduna M, et al. Intimate partner violence, relationship power inequity, and incidence of HIV infection in young women in South Africa: a cohort study. Lancet. 2010;376:41–48. 8. Kouyoumdjian FG, Calzavara LM, Bondy SJ, et al. Intimate partner violence is associated with incident HIV infection in women in Uganda. AIDS. 2013;27:1331–1338. 9. Mulrenan C, Colombini M, Howard N, et al. Exploring risk of experiencing intimate partner violence after HIV infection: a qualitative study among women with HIV attending postnatal services in Swaziland. BMJ Open. 2015;5:e006907. 10. Shamu S, Zarowsky C, Shefer T, et al. Intimate partner violence after disclosure of HIV test results among pregnant women in Harare, Zimbabwe. PLoS One. 2014;9:e109447. 11. Brooks R, Jolly P, Marsh L, et al. Intimate partner violence among HIV-positive women in Nairobi, Kenya. Int J Women's Health. 2019;11:451–461. 12. Tsai AC, Wolfe WR, Kumbakumba E, et al. Prospective study of the mental health consequences of sexual violence among women living with HIV in rural Uganda. J Interpers Violence. 2016;31:1531–1553. 13. Houry D, Kemball R, Rhodes KV, et al. Intimate partner violence and mental health symptoms in African American female ED patients. Am J Emerg Med. 2006;24:444–450. 14. Eisinger RW, Dieffenbach CW, Fauci AS. HIV viral load and transmissibility of HIV infection: undetectable equals untransmittable. JAMA. 2019;321:451–452. 15. Baeten JM, Donnell D, Ndase P, et al. Antiretroviral prophylaxis for HIV prevention in heterosexual men and women. New Engl J Med. 2012;367:399–410. 16. Siemieniuk RA, Krentz HB, Miller P, et al. The clinical implications of high rates of intimate partner violence against HIV-positive women. J Acquir Immune Defic Syndr. 2013;64:32–38. 17. Trimble DD, Nava A, McFarlane J. Intimate partner violence and antiretroviral adherence among women receiving care in an urban Southeastern Texas HIV clinic. J Assoc Nurses AIDS Care. 2013;24:331–340. 18. Rubtsova A, WingoodDunkle GK, Camp C, et al. Young adult women and correlates of potential adoption of pre-exposure prophylaxis (PrEP): results of a national survey. Curr HIV Res. 2013;11:543–548. 19. Willie TC, Stockman JK, Overstreet NM, et al. Examining the impact of intimate partner violence type and timing on pre-exposure prophylaxis awareness, interest, and coercion. AIDS Behav. 2018;22:1190–1200. 20. Roberts ST, Haberer J, Celum C, et al. Intimate partner violence and adherence to HIV pre-exposure prophylaxis (PrEP) in African women in HIV serodiscordant relationships: a prospective cohort study. J Acquir Immune Defic Syndr. 2016;73:313–322. 21. Cabral A, M Baeten J, Ngure K, et al. Intimate partner violence and self-reported pre-exposure prophylaxis interruptions among HIV-negative partners in HIV serodiscordant couples in Kenya and Uganda. J Acquir Immune Defic Syndr. 2018;77:154–159. 22. Heffron R, Muwonge TR, Thomas KK, et al. PrEP uptake and HIV viral suppression when PrEP is integrated into Ugandan ART clinics for HIV-negative members of HIV-serodifferent couples: A stepped wedge cluster randomized trial. EClinicalMedicine. 2022;52:101611. 23. Cherpitel CJ. A brief screening instrument for problem drinking in the emergency room: the RAPS4. Rapid alcohol problems screen. J Stud Alcohol. 2000;61:447–449. 24. Castillo-Mancilla JR, Searls K, Caraway P, et al. Short communication: tenofovir diphosphate in dried blood spots as an objective measure of adherence in HIV-infected women. AIDS Res Hum Retroviruses. 2015;31:428–432. 25. Castillo-Mancilla J, Seifert S, Campbell K, et al. Emtricitabine-triphosphate in dried blood spots as a marker of recent dosing. Antimicrob Agents Chemother. 2016;60:6692–6697. 26. Zheng J-H, Rower C, McAllister K, et al. Application of an intracellular assay for determination of tenofovir-diphosphate and emtricitabine-triphosphate from erythrocytes using dried blood spots. J Pharm Biomed Anal. 2016;122:16–20. 27. Donnell D, Baeten JM, Bumpus NN, et al. HIV protective efficacy and correlates of tenofovir blood concentrations in a clinical trial of PrEP for HIV prevention. J Acquir Immune Defic Syndr. 2014;66:340–348. 28. Straus MA, Gelles RJ, Asplund LM. Physical Violence in American Families: Risk Factors and Adaptations to Violence in 8,145 Families. New Brunswick, NJ: Transaction Publisher; 1990. 29. Ashburn K, Kerner B, Ojamuge D, et al. Evaluation of the responsible, engaged, and loving (REAL) fathers initiative on physical child punishment and intimate partner violence in Northern Uganda. Prev Sci. 2017;18:854–864. 30. Wagman JA, Gray RH, Campbell JC, et al. Effectiveness of an integrated intimate partner violence and HIV prevention intervention in Rakai, Uganda: analysis of an intervention in an existing cluster randomised cohort. Lancet Glob Health. 2015;3:e23–e33. 31. Pulerwitz J, Gortmaker SL, DeJong W. Measuring sexual relationship power in HIV/STD research. Sex Roles. 2000;42:637–660. 32. Closson K, Dietrich JJ, Beksinska M, et al. Measuring sexual relationship power equity among young women and young men South Africa: implications for gender-transformative programming. PLoS One. 2019;14:e0221554. 33. Zembe YZ, Townsend L, Thorson A, et al. Intimate partner violence, relationship power inequity and the role of sexual and social risk factors in the production of violence among young women who have multiple sexual partners in a peri-urban setting in South Africa. PLoS One. 2015;10:e0139430. 34. Hatcher AM, Tsai AC, Kumbakumba E, et al. Sexual relationship power and depression among HIV-infected women in rural Uganda. PLoS One. 2012;7:e49821. 35. R: A Language and Environment for Statistical Computing [computer Program]. Version 4.2.2. Vienna, Austria: R Foundation for Statistical Computing; 2023. 36. Hampanda KM. Intimate partner violence and HIV-positive women's non-adherence to antiretroviral medication for the purpose of prevention of mother-to-child transmission in Lusaka, Zambia. Soc Sci Med. 2016;153:123–130. 37. Hatcher AM, Smout EM, Turan JM, et al. Intimate partner violence and engagement in HIV care and treatment among women: a systematic review and meta-analysis. AIDS.
留言 (0)