To the best of our knowledge, this is the first study evaluating clinical factors predictive of CKD stage 4–5 post-SABR for primary RCC. It is also one of the largest single institution series of renal SABR reported to date. Our series demonstrates post-treatment deterioration in renal function comparable to published surgical series despite our older cohort (median age of 77.8 years vs. 60–65 in most surgical series) and relatively lower baseline eGFR. Baseline CKD stage remained the only predictive factor on multivariable analysis with 1/35 (2.8%) of patients with baseline CKD stage 1–2 progressed to stage 4 at the last follow-up, with no patients developing ESRD.
The incidence of early-stage renal cell carcinoma (RCC) has increased over the last 3 decades, alongside a concomitant decrease in mortality of RCC as a whole [12]. Considering the excellent long-term oncological outcomes of early stage RCC, recent focus has shifted towards maintaining quality of life (QOL) through the reduction of treatment-related morbidity, in particular renal function preservation. Chronic kidney disease (CKD) is associated with a higher risk of death, cardiovascular events, and hospitalization. In a large population-based study, estimated glomerular filtration rates (eGFR) of 15–29 and < 15 ml/min were associated with age-adjusted mortality rates of 11.4 and 14.1 per 100 person-years, respectively [13]. It is therefore crucial to limit CKD progression following treatment for localized early-stage RCC.
Multiple studies have addressed CKD progression post-surgery in patients with baseline CKD stage 1–2 and reported better outcomes with PN. A large Canadian retrospective series by Mason et al. reported 2.1% (10/466) and 5.4% (29/532) of patients with baseline CKD stage 1–2 progressing to stage 4–5 following PN and RN, respectively [9]. Similar findings were found in another large retrospective study in RCC patients with baseline CKD stage 2 (CKD stage 4–5: 2.7% in PN and 4.3% in RN) [14]. In the only randomized trial of RN versus PN (EORTC 30904), postoperative incidence of CKD stage 4–5 incidence was significantly lower in the PN group (6.3% vs. 10.0%) [15].
In previously reported surgical series, preoperative CKD stage was significantly associated with post-operative CKD progression [9, 16]. Mason et al. reported worse progression with increasing CKD stage for patients treated with both PN and RN—in patients with CKD stage 2 at baseline, eGFR fell below 30 in 8.4% of the RN and 3% of the PN group at last follow-up, but 43.2% (60/139) and 19.4% (18/93) of patients with baseline CKD stage 3 progressed to stage 4–5 following RN and PN, respectively [9]. In our study, baseline CKD stage was also the strongest predictor of progression to stage 4–5 on univariable and multivariable analysis, with stage 3b patients faring the worst—83.9% developed CKD stage 4–5 by their last follow up. The interpretation of this is challenging as the natural history of CKD is highly variable even in the absence of renal cell carcinoma; CKD progression risk does however seem to be higher in stage 3b patients compared to patients with earlier stage disease [17,18,19]. Our cohort shows that whilst the general trend was for a decline in renal function over time following SABR, 13/78 patients (17%) had a final eGFR higher than the baseline eGFR. However, this was marginal—the increase in eGFR was < 5 in all but 3 patients (pre-SBRT eGFR 49,45 and 70), which might be due to compensatory responses from the remaining functional nephrons.
Patients with baseline CKD stage 3b and primary RCC present a significant dilemma to the treating physician. Any intervention has the potential to significantly accelerate renal function decline in this already high-risk cohort. One study by Takagi et al. reported no significant difference in development of new onset CKD stage 4–5 in patients with base line CKD 3b at 2-years with PN (55%) over RN (46%) [20]. In our study, we also found an ongoing decline of renal function following SABR for patients with baseline CKD 3b, with 1- and 5-year freedom from CKD stage 4–5 development of 58.1% and 16.4%, respectively. Four patients (all stage 3b at baseline) progressed to ESRD at last follow up, consistent with the long-term follow-up results post SABR for RCC previously reported by Siva et al. [4]. In that study, 3.7% (7/190) patients with mean ± SD baseline eGFR of 32.8 ± 13.2 mL/min, underwent dialysis post-SABR. Therefore, early education is paramount in this high-risk RCC cohort to ensure that they are adequately informed to make the appropriate choices, including the option of best supportive care. Irrespective of treatment modality, patients in this group should be offered early nephrology referral for regular monitoring and intervention to slow the progression of renal function decline and management of CKD-related complications.
Whilst increasing age, hypertension, diabetes mellitus and tumor size have been linked with greater loss in renal function and progression to CKD stage 4–5 in surgical series [6,7,8, 21], these factors were not significant contributors to renal function loss in this study. This might be due to a smaller sample size, older population or poorer baseline renal function at the time of SABR in this study compared to previous surgical series, overwhelming the impact of comorbidity on post-treatment renal function. It may also reflect the different pathogenesis of nephropathy post-surgery and radiotherapy. However, similar findings were reported in prior radiotherapy studies as well. In one study, Park et al. [22] found only baseline eGFR to be the sole prognostic factor for renal function impairment in their multivariable logistic regression analysis when evaluating the risk factors for renal function impairment in patients with gastric cancer treated with surgery and adjuvant radiotherapy.
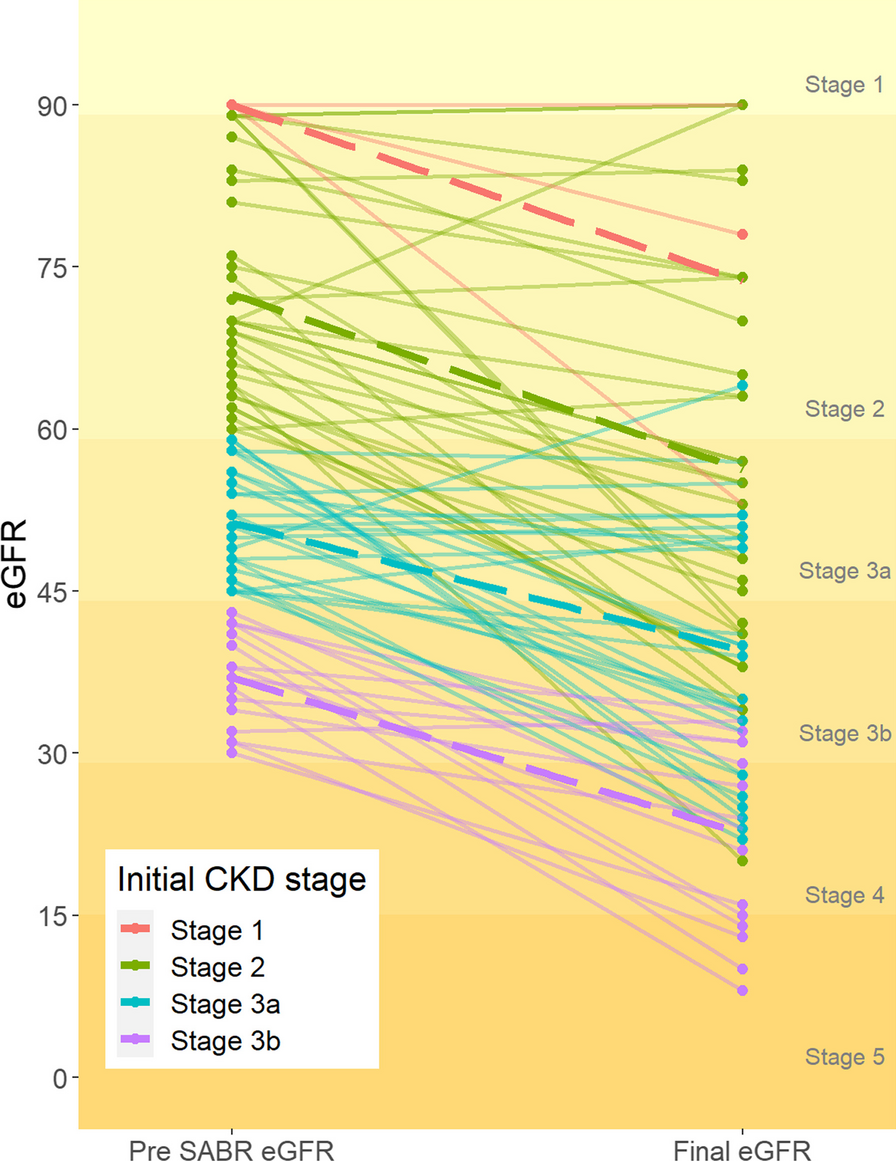
Renal parenchyma loss remains the main cause of renal function decline post-PN, but renal ischemia secondary to renal artery clamping during surgery is also a contributing factor, with prolonged ischemia time associated with more postoperative renal function decline [23, 24]. Diabetes has been demonstrated to increase reperfusion injury following ischemia in a rodent model [25] and whilst the aetiopathogenesis of renal failure in the setting of hypertension following renal artery clamping is less clear, there are well appreciated complex interactions between hypertension and renal ischemia [26]. By comparison, radiation nephropathy results in cell death through the dose-dependent creation of double-stranded DNA breaks [27]. There should in theory be no effect on nephrons not receiving a significant radiation dose and the severity of radiation nephropathy therefore depends on the total dose and the kidney volume being irradiated [27, 28]. The steep dose gradient in SABR limits the volume of irradiated normal tissue and results in reduced radiation dose to normal renal parenchyma. This is consistent with our observation that there is an almost identical decline in mean eGFR in our cohort, irrespective of baseline CKD stage (Fig. 1).
In this study, the single fraction SABR regimen was associated with a lower incidence of CKD stage 4–5 compared to multi-fraction SABR on univariable analysis (p = 0.005), though this did not reach statistical significance on multivariable analysis. Whilst we cannot draw firm conclusions from the data due to sample size and imbalances between fractionation groups, we might hypothesise that the lower total dose used in single fraction SABR results in reduced dose to normal renal parenchyma compared to multi-fraction, better preserving renal function. In one study, Siva et al. [29] reported that limiting the volume of kidney receiving > 50% prescription dose may reduce the risk of renal function loss and this is backed up by Yamamoto et al. [30] who found strong correlations between the dose distribution of 20 and 30 Gy and renal atrophy in patients receiving SABR. The choice of fractionation schedule is however heavily confounded by other factors, including age, tumour size and baseline CKD status. Further investigation of the impact of fractionation schedule on CKD progression is necessary, especially considering previous work showing worse local failure and progression free survival in multi-fraction SABR schedules [4].
Despite being the first study of its kind, there are also a few limitations. (1) This is a retrospective study. (2) Our sample size is relatively small compared to most published surgical series. Both limitations result from the novelty of SABR as a treatment modality for localised primary RCC and limited indications for its use in patients who are medically inoperable or at high risk of dialysis post-surgery. (3) Renal parenchyma dosimetry data is not presently available for these patients.
To address these limitations, we have established an international prospective registry on the platform of International Radiosurgery Oncology Consortium for Kidney cancer (IROCK), which will continue to collect prospective data (https://www.irockregistry.com/). We are also ensuring that dosimetry data is included for this ongoing project. In planning for future randomised trials, the effect of single vs multifraction SABR should be considered, with tumor related outcomes and renal function changes as co-endpoints.





留言 (0)