
記住我
Appendicectomy is amongst the most commonly performed surgery, with acute appendicitis being the most frequent reason for abdominal surgical emergencies in the world.1 The lifetime risk of appendicitis is 7–8%, with rising incidence in the newly industrialised countries.2,3 The prevailing treatment of choice for appendicitis is appendicectomy, which can be performed either ‘open’ or laparoscopically.4
Although often characterised as minor or less invasive operations, appendicectomies, open or per laparoscopy, are still a cause of significant postoperative pain. Gerbershagen et al.5 have shown high pain scores on the first postoperative day, with a median score of 5 of 10 for laparoscopic and 6 of 10 for open appendicectomies, placing them within the same range as knee joint replacements and sternotomies. This may result from underestimating pain after more minor surgery leading to a limitation of pain management and undertreatment. In addition, appendicectomies are often associated with inflammatory processes, which produce pain in addition to the surgical injury. In addition to the improvement of patients’ satisfaction, adequate pain management after surgery decreases the length of hospital stay, reduces the risk of chronic postoperative pain, as well as morbidity and mortality.6–10 Particularly, in view of the ongoing discourse surrounding same-day appendicectomies, the provision of effective pain management holds significant importance.11 Appropriate pain therapy is, therefore, imperative for all surgery, including the so-called ’minor operations’ like appendicectomies.
To develop evidence-based recommendations for pain management specific for each surgical procedure, a collaboration of surgeons and anaesthetists have established a Working Group named PROSPECT (PROcedure-SPECific postoperative pain managemenT).12
The recommendations are based on systematic reviews of randomised controlled trials, systematic reviews and meta-analyses. The methodology includes a Delphi process that takes clinical practice, efficacy and adverse effects of each potential analgesic technique into consideration.13
This systematic review aims to assess the available literature on the effects on pain of analgesics, anaesthetics and surgical interventions after both open and laparoscopic appendicectomy. The primary outcome was postoperative pain intensity. Secondary outcomes, including rescue analgesics, the time to recovery and adverse effects, were addressed when reported, and the limitations of the data were reviewed. Depending on the extent of evidence, the intention was ultimately to develop recommendations for pain management concerning appendicectomies.
MethodsThis review's methods were established prior to its conduct and followed the PROSPECT methodology.14 Five electronic databases (PubMed, Embase, Ovid MEDLINE, Cochrane Database of Systematic Reviews and Cochrane Central Register of Controlled Trials) were searched using the PRISMA (Preferred Reporting Items for Systematic Reviews and Meta-Analysis) search protocols to identify randomised controlled trials published in the English language from January 1999 up to October 2022.15 The study design of randomised controlled trials was selected because of their strong evidence and, following the Consolidated Standards of Reporting Trials (CONSORT) guidelines, relatively low bias.16
We used a search string with a sequence of Medical Subject Heading (MeSH) terms, text words and word variants related to appendicectomy pain management (Supplement Table 1, https://links.lww.com/EJA/A913). Two authors (SB and JF) conducted the literature search, screening and excluding irrelevant articles independently. The reference lists of retrieved reviews, systematic reviews and meta-analyses were hand-searched for additional relevant studies. After comparing their initial screening results, any disagreements were resolved by consensus between reviewers. In the case of any discrepancies, a third reviewer (EM P-Z) collaborated for a final decision.17
Studies of the adult and paediatric population were included. Articles reporting combined data from patients undergoing mixed surgical procedures were only included if data specific for appendicectomies were available for extraction. In addition, studies had to state pain intensities measured by a visual analogue scale (VAS) or a numerical rating scale (NRS). Studies that did not report on the precise operative technique of appendicectomy were excluded. The criteria are summarised in Supplement Table 2, https://links.lww.com/EJA/A914 following the Patient Intervention Comparison Outcome (PICO) system.18 Studies in children and adults were included, as well as mixed patients related to age. Initially, studies in children and adults were analysed separately, with ages 15 and above considered adults.
Quality assessment, including risk of bias assessment, using the Version 2 of the Cochrane risk-of-bias tool, as well as data extraction and analysis, was performed in accordance with the PROSPECT methodology.14
The primary objective of this analysis was postoperative pain intensity. A change of more than 10 mm on a 100 mm VAS or NRS was considered clinically relevant.19 Secondary objectives included postoperative analgesic consumption, available baseline analgesia, time to first analgesic consumption, the effect on the incidence of postoperative nausea and vomiting (PONV), the impact on the time to return to work or normal activities, length of hospital stay, the duration of operation, the duration of anaesthesia and postoperative complications. We defined adequate baseline analgesia as any routinely given nonopioid analgesic; for example, paracetamol, nonsteroidal anti-inflammatory drugs (NSAID) and selective cyclooxygenase-2 inhibitor (COXIB).
The aim of this review was not to perform a meta-analysis but to assess the data qualitatively. The literature search results were presented and discussed initially in the appendicectomy PROSPECT subgroup and the first formulation of recommendations according to the prospect methodology.14 Briefly, the validity of each intervention investigated in the included studies was qualitatively assessed by the number of studies showing a significant and clinically relevant difference. The minimum requirement for a recommendation was at least two congruent studies supporting the analgesic technique in question with statistically significant and clinically relevant results (primary outcome, pain intensity; secondary outcome, rescue analgesia requirement). The risks and benefits of each analgesic technique, the quality of the studies and the presence of a baseline pain treatment were considered while developing the final recommendations. The proposal of all recommendations and the underlying literature/summary of results from each study was subsequently submitted to the entire PROSPECT Working Group, followed by virtual round-table discussions and an exchange of expert opinions. Efficacy was weighed against side effects and risks of treatment and discussed between all PROSPECT members. Once a consensus had been obtained, the lead authors drafted the final document, which finally required the Working Group's approval using the Delphi technique.20
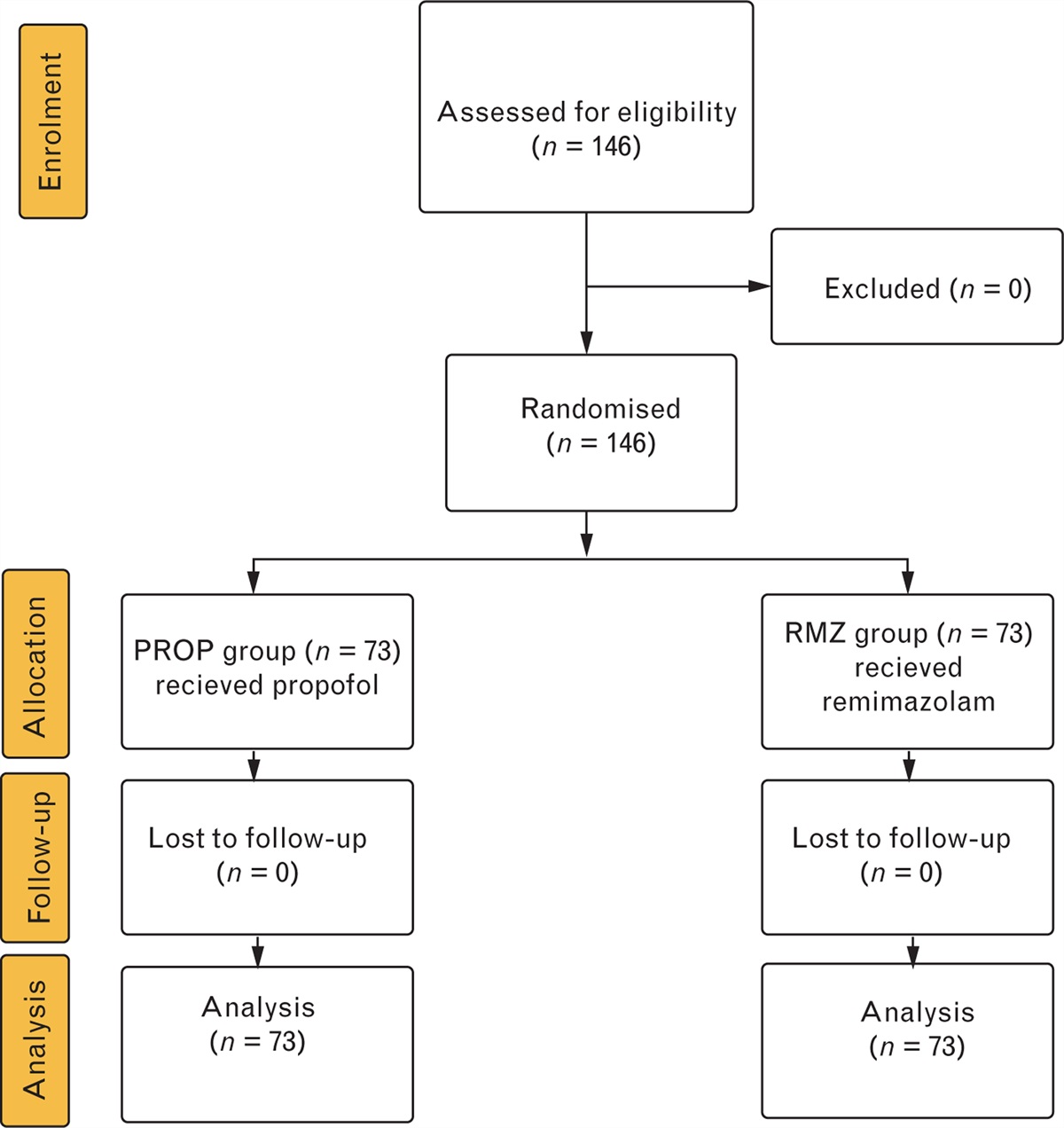
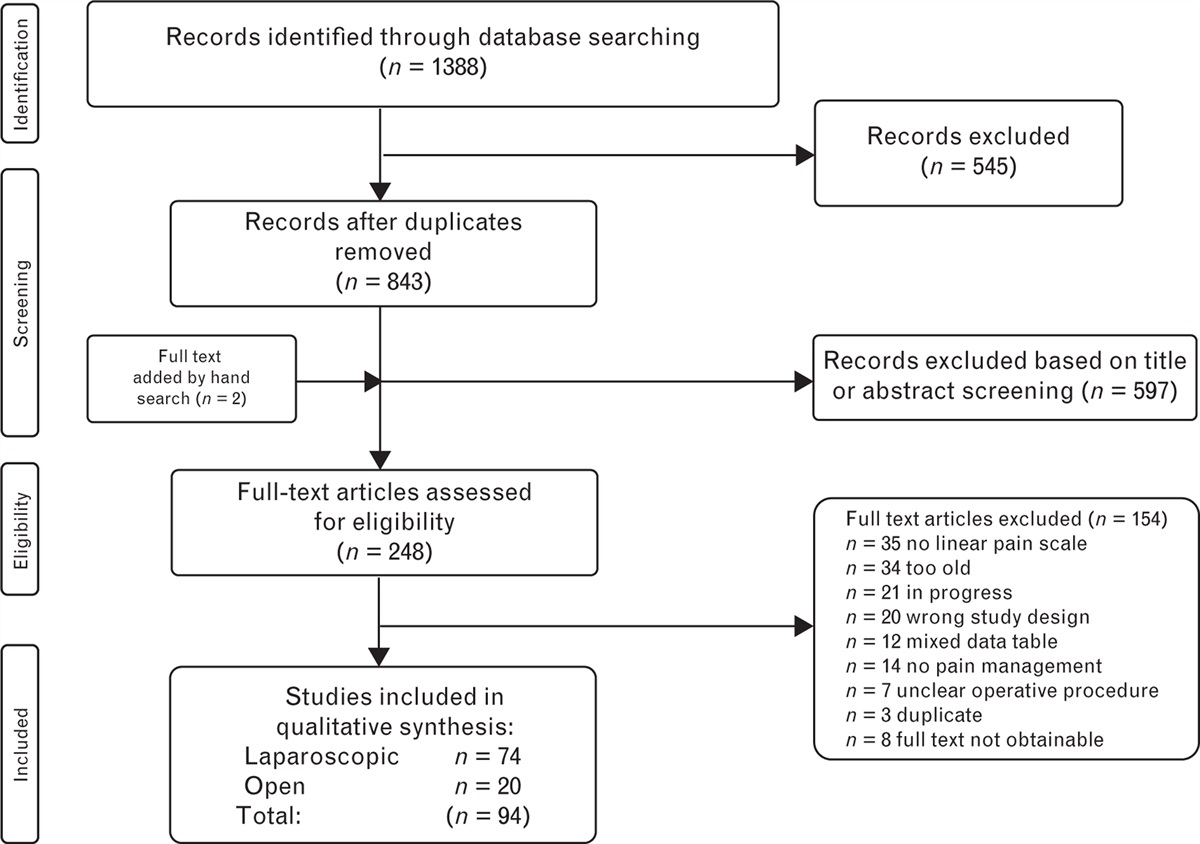
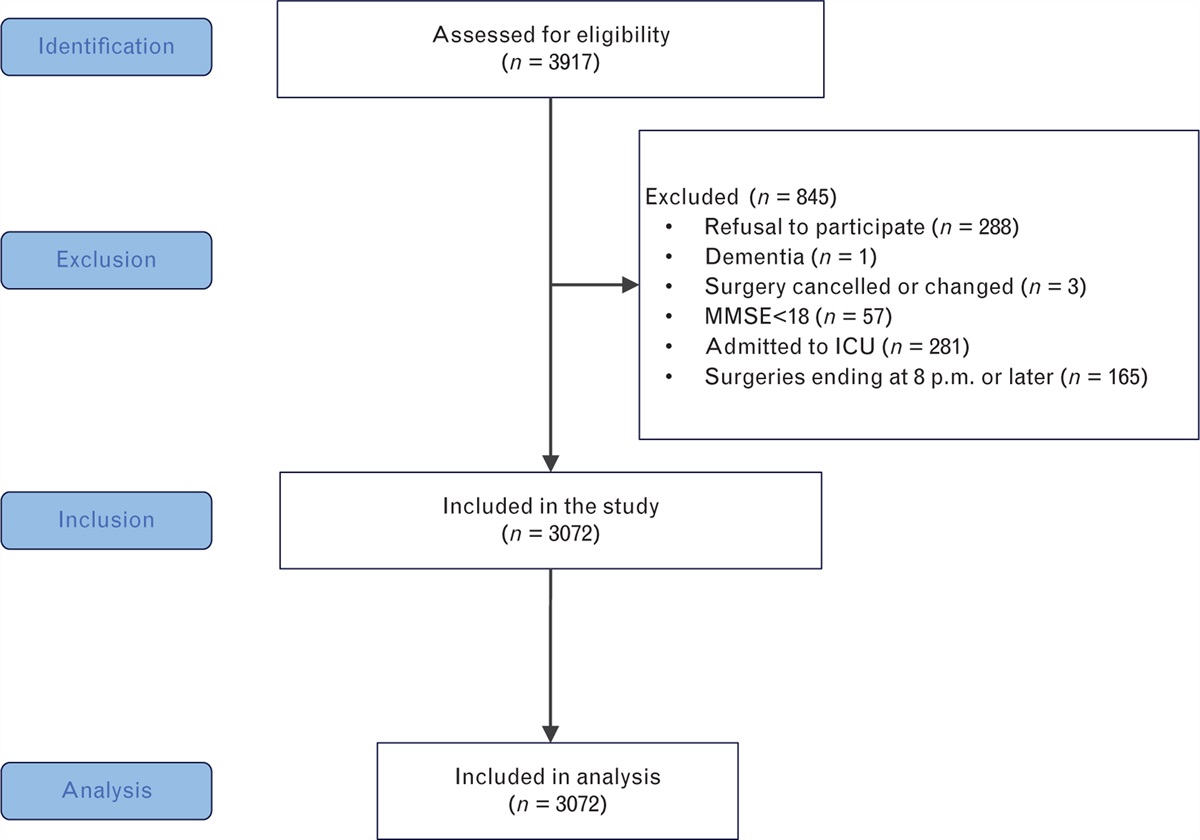
ResultsThe systematic literature search identified a total of 1388 records. After excluding duplicates and studies not fulfilling the inclusion criteria, 94 studies were included in the qualitative analysis (see Figure 1: PRISMA flow chart for inclusions and exclusion). The methodological quality assessments and the characteristics of the studies included are compiled in Supplement Table 3, https://links.lww.com/EJA/A915. Among the selected studies, 53 included adult, 20 paediatric patients, and 21 involved a mixed population. The definition of adult and paediatric populations showed variations among the studies. We considered the population as adults if the patients were 15 years or older. However, the average age of children was about 12 years without infants being included; accordingly, pain was assessed similarly as in adults. Additionally, surgical procedures in adults and children did not differ (although open appendicectomies are more often required in children than in adults). Thus, the PROSPECT working group agreed that the results of studies including children, although analysed separately from adult studies, should be analysed together with results from studies in adults (and mixed populations). However, laparoscopic and open surgical procedures were analysed separately, and recommendations were made accordingly.
 Fig. 1:
Fig. 1: Prisma flow chart for inclusion and exclusion.
Surgical technique for appendicectomy Three-port laparoscopic appendicectomy versus open appendicectomy?????
Adult patientsThirteen randomised controlled trials, including 2079 patients, compared conventional three-port laparoscopic appendicectomy to open appendicectomy in adults.21–33 Eight of them utilised adequate baseline analgesia.21–23,28,29,31–33 Out of the thirteen studies retrieved, four did not find a difference in pain intensity,21,24,27,33 and one demonstrated a significantly lower pain score in favour of open appendicectomy.30 The remaining eight studies recorded a significant benefit on pain intensity ratings for patients undergoing conventional three-port laparoscopic appendicectomy, with five showing an additional significant reduction in analgesic consumption.22,23,29,31,32 The maximum duration of pain intensity reduction was reported by Jan and colleagues, lasting two weeks postoperatively.25 Concerning complications, the open appendicectomy group had a significantly higher rate in four studies, with the remaining studies showing no significant difference.25,28–30
Two systematic reviews and meta-analyses showed a significantly reduced pain intensity advocating conventional three-port laparoscopic appendicectomy.34,35
Additional four studies with a mixed population and average ages in adulthood further report a significantly reduced pain intensity.36–39 Out of them, Rashid et al. and Singh et al. reported a clinically relevant reduction in pain with Rashid's study using adequate baseline analgesia.37,39
Out of four systematic reviews and meta-analyses with mixed populations,40–43 three reported significantly reduced pain intensity in patients undergoing conventional three-port laparoscopic appendicectomy.41–43 The remaining study by Wei et al. showed a significantly shorter length of analgesia (days of medication given) attributed to conventional three-port laparoscopic appendicectomy.40
Paediatric patientsIn the paediatric population, one study by Lintula and colleagues reported a statistically significant postoperative reduction in pain intensity ratings at eight hours after laparoscopic compared with open appendicectomy with adequate opioid-sparing baseline analgesia.44
Sauerland and colleagues’ systematic review and meta-analysis concluded that the evidence is too limited and inconsistent to formulate a statement concerning pain intensity for the paediatric population.34 This review from 2010 was updated by Jaschinski et al. in 2018 but found no additional evidence.35
Single- versus three-port incisional laparoscopic appendicectomyThirteen studies (seven in adults,23,45–50 four with a mixed population39,51–53 and two in children)54,55 investigated the efficacy of single-incision laparoscopic appendicectomy compared with conventional three-port laparoscopic appendicectomy.
Adult patientsIn the adult population, three of the included studies showed significantly lower pain scores for single-incision laparoscopic appendicectomy,47–49 with two reporting a clinical relevance combined with adequate baseline analgesia.48,49 Exclusively, Teoh's trial additionally demonstrated significantly lower analgesic use.49 Three studies reported no difference in pain intensity and analgesic consumption.23,45,46 One trial by Carter and colleagues showed a significantly higher pain intensity for single-incision laparoscopic appendicectomy with significantly increased opioid consumption but without adequate baseline analgesia.50 Four systematic reviews and meta-analyses displayed no significant benefit in pain intensity attributed to single-incision laparoscopic appendicectomy compared with conventional three-port laparoscopic appendicectomy.56–59
Mixed populationThe studies by Singh et al. and Duza et al., examining a mixed population, included patients between 12 and 50 years and 14 and 65 years, respectively.39,51 Duza's study reports a clinically relevant reduction in pain without opioid-sparing effect or adequate baseline analgesia.51 Singh et al. reported no difference in pain scores or analgesic consumption.39 None of the previous trials reported significant complications assigned to single-incision laparoscopic appendicectomy.
Multiple systematic reviews and meta-analyses displayed no significant benefit in pain intensity and analgesic requirements attributed to single-incision laparoscopic appendicectomy compared with conventional three-port laparoscopic appendicectomy.52,60–66
Paediatric patientsOut of the two trials in the paediatric population, one reported significantly increased pain intensity ratings and opioid consumption associated with single-incision laparoscopic appendicectomy.55 In both studies, baseline analgesia was administered. Binet and colleagues’ study with the addition of a rectus sheath block for all patients demonstrated a clinically significant reduction of pain intensity for a limited time in the recovery room.54
Regional analgesia techniques Transverse abdominis plane blockTwelve studies (three for laparoscopic appendicectomy in adults,67–69 one for open appendicectomy in adults,70 one for laparoscopic in children,71 and seven for open appendicectomy in children)72–78 assessed the analgesic effect of transverse abdominis plane (TAP) block. Eleven out of the twelve studies included adequate baseline analgesia.
Laparoscopic appendicectomy: adult populationIn two studies assessing the efficacy of a TAP block in the adult population undergoing laparoscopic appendicectomies, the TAP blocks were performed bilaterally and preoperatively. Tanggaard et al. compared a dual bilateral TAP block with 0.375% ropivacaine (15 ml each site, 60 ml in total) to a TAP block with 0.9% saline, demonstrating a statistically and clinically significant reduction of pain intensity during sitting and statistically significant at rest in the first 12 h postoperatively.67 There was no effect on opioid consumption. Tupper-Carey et al. compared a TAP block using 20 ml of 0.5% ropivacaine on each side with 0.9% saline port site infiltration versus port site infiltration with 10 ml of 0.5% bupivacaine but without TAP block.68 Pain intensity ratings were similar in both groups except at 36 h postoperatively (pain intensity at rest); there was no opioid-sparing effect.
Both studies used adequate baseline analgesia and reported no adverse effects associated with performing the TAP block.
An additional study by Sertcakacilar et al. compared the efficacy of ultrasound-guided transversus abdominis plane block to lateral approach quadratus lumborum block. Both blocks were performed bilaterally with 20 ml of 0.375% bupivacaine, showing no significant difference in pain intensity ratings.69
Laparoscopic appendicectomy - paediatric populationSandemann et al. compared preoperative bilateral TAP block using 0.5 ml kg−1 of 0.2% ropivacaine in each site combined with port-site infiltration using 0.5 ml kg−1 of 0.2% ropivacaine to solely port-site infiltration.71 Both groups received adequate baseline analgesia. The analgesic benefit was limited and showed a clinically significant pain reduction exclusively at the recovery ward with no difference in opioid requirements and adverse events.
Open appendicectomy: adult populationThere was no study investigating TAP blocks in adults for open appendicectomy. Ghimire and colleagues’ three-arm study examined the effect of morphine added to bupivacaine (either as an adjuvant in the TAP block or as intravenous morphine).70 Even though there was a significantly longer mean duration of analgesia measured by the time to first analgesic request in the group receiving morphine as an adjuvant, there was no significant reduction in pain intensity or opioid consumption. All groups received baseline analgesia.
Open appendicectomy: paediatric populationOut of the seven studies retrieved, three compared TAP block to no block,73,74,77 two compared TAP block to placebo ('sham’ TAP block),72,76 one compared TAP block to local wound infiltration,78 and one examined different dosing of ropivacaine used for TAP block.75 All TAP blocks were performed unilaterally, utilising bupivacaine or ropivacaine as local anaesthetics. Except for Jalil et al.,75 comparing different doses of ropivacaine, all studies reported adequate baseline analgesia. All but one77 showed a statistically and clinically significant pain reduction by use of the TAP block. Ghimire, as well as Patel and colleagues, demonstrated a reduction of pain lasting 12 h postoperatively.72,73 There was a prolonged reduction in pain described by Shaaban and Carney et al. lasting up to 18 h. Niraj et al. show the same effect continuing up to 24 h postoperatively.74,76,78 All but one study,77 with no significant effect on pain scores, displayed a significant reduction in opioid consumption. None of the studies reported significant complications attributed to the TAP block; most were of good quality with adequate allocation concealment.
Intraperitoneal local anaestheticsSeven studies, including 679 patients, assessed the effectiveness of intraperitoneal applied local anaesthetics in laparoscopic appendicectomies, five studies79–83 regarding adults and two concerning children.84,85
Laparoscopic appendicectomy: adult populationNone reported or specified their baseline analgesia or complications associated with the investigated intervention from the five studies in adults.79–83 Thanapal's79 study compared ropivacaine and levobupivacaine to 0.9% saline installation into the right paracolic gutter, caecum and appendix site. Although pain intensity scores were reported, they could not be factored in as the PCA with morphine targeted a VAS score of 0 to 1 using rescue analgesia. In the two groups using differing local anaesthetics, the morphine consumption was significantly decreased compared with the placebo group but without a significant difference between them.
Sevensma et al.80 compared the use of 20 ml of 0.5% bupivacaine to 0.9% saline at the appendix site and showed reduced pain intensity scores up to 12 h but clinically relevant only for the first hour postoperatively. The opioid requirement, converted to equivalent intravenous morphine sulphate doses, was significantly reduced for the bupivacaine group.
Kang et al.81 investigated the effect of instilling 2 mg kg−1 of ropivacaine compared with 0.9% saline on the liver's upper surface, the right subdiaphragmatic space and the appendix site. During the 48 h postoperative period, all patients in the ropivacaine group showed a significantly reduced pain score, except at 24 h. Clinically significant pain reduction lasted until 8 h postoperatively. Accordingly, fentanyl consumption was significantly reduced in the ropivacaine group.
A three-arm study by Kim et al.82 compared the intraperitoneal and intravenous application of lidocaine to a 0.9% saline placebo. Lidocaine (3.5 mg kg−1) was sprayed on the liver's upper surface, under the right and left subdiaphragmatic space and at the appendicectomy site. The group receiving intravenous lidocaine had a bolus of 1.5 mg kg−1 lidocaine administered before intubation, followed by continuous infusion at 2 mg kg−1 h−1 of lidocaine. The intraperitoneal group had a clinically significant reduction of pain scores until 12 h postoperatively compared with the placebo group. The intravenous group also had significant pain reduction lasting 8 h postoperatively but without clinical significance. Between both intervention groups, there was no significant difference in pain intensity. Fentanyl consumption was significantly less in the intraperitoneal and intravenous group compared with the placebo group and significantly less in the intraperitoneal group than in the intravenous group.
Custovic et al.83 investigated peritoneal and port-site infiltration with different local anaesthetics compared with a placebo group. Three local anaesthetics were tested, lidocaine 1%, levobupivacaine 0.5% and ropivacaine 0.5%. In each group, 5 ml of the local anaesthetic was applied at the incisional site and 10 ml under direct vision in the right iliac fossa area, around the appendix site and at the trocar sites at the end of the procedure. Compared with the control group, the average pain intensity in the levobupivacaine and ropivacaine groups was clinically significantly reduced. The lidocaine group's pain intensity was decreased compared with the control group but failed to reach a significant and clinically relevant level.
Laparoscopic appendicectomy: paediatric populationHamill et al.84 compared the application of 20 ml of 0.25 or 0.125% bupivacaine, depending on weight, onto the peritoneum of the right iliac fossa and pelvis to application of 0.9% saline. There was neither a reduction in VAS score nor a decrease in opioid consumption. Both studies used adequate baseline analgesia and described no complications associated with performing the interventions.
Elnabtity and Ibrahim85 compared intraperitoneal administration of 0.25% bupivacaine with 0.9% saline to the same dose of bupivacaine combined with dexmedetomidine 1 μg kg−1 diluted in 5 ml of 0.9% saline. The group with added dexmedetomidine had a significantly lower median VAS score at 2, 4, and 6 h postoperatively, which reached clinical and statistical significance. A significant reduction in pethidine requirements was also noted.
Laparoscopic appendicectomy: mixed populationOne systematic review and meta-analysis by Abdelhakim et al.86 with a mixed population (one paediatric and six adult studies) investigated the effect of intraperitoneal local anaesthetic in laparoscopic appendicectomy. They demonstrated a significant analgesic benefit in the intraperitoneal group at 8, 12, and 24 h postoperatively with an opioid-sparing effect. Correspondingly the incidence of PONV, shoulder pain and the length of hospital stay were reduced.
Wound infiltrationSeven studies investigated the effect of local wound infiltration, including 532 patients: one study for single-incision laparoscopic appendicectomy in adults;87 three studies for open appendicectomy in adults,88–90 two studies for open appendicectomy in children91,92 and one study concerning open appendicectomies in a mixed population.93
Single-incision laparoscopic appendicectomy: adult populationHa and colleagues compared preoperative periumbilical infiltration with bupivacaine to saline infiltration during single-incision appendicectomy. They demonstrated a reduced opioid consumption but did not observe a significant pain reduction, while using adequate baseline analgesia. No significant adverse effects were reported.87
Open appendicectomy: adult populationAnsaloni et al.88 compared continuous wound instillation via an elastomeric infusion pump device filled with either 0.2% ropivacaine or 0.9% saline for 2 days following surgery. They demonstrate a significant postoperative pain reduction in the intervention group for 36 h with clinically relevant effects at three hours and 24 h and a decreased analgesic consumption. Adequate baseline analgesia was administered. No significant adverse effects were reported.
Likewise, Refaat et al. compared preoperative local subcutaneous infiltration (method A) versus subcutaneous and deep to external oblique infiltration (method B) with 0.25% bupivacaine; both compared with a control group (method C).89 In method B the pain scores were clinically significantly reduced compared with method A and C in the first 24 h postoperatively, except at 8 h when the control group was almost equal to method B. Only in the first postoperative hour did method A show a significant pain reduction compared with the control group. The pethidine requirement was significantly lower only in method B, but no adequate baseline analgesia was reported.
Lohsiriwat et al.90 compared preoperative use of 10 ml of 0.5% bupivacaine infiltrated into the skin and subcutaneous tissue against no intervention, showing significantly lower pain scores in the bupivacaine group until 24 h postoperatively, with a clinical significance lasting up to 12 h. The morphine consumption was significantly less in the intervention group while using adequate standard analgesia. There was no complication reported.
Open appendicectomy: paediatric populationA three-arm study by Edwards et al.91 assessed the effectiveness of local anaesthetic wound infiltration with 0.5 ml kg−1 of 0.25% bupivacaine to 0.5 ml kg−1 of 0.9% saline compared with no infiltration in the presence of adequate baseline analgesia. Neither a significant difference in pain intensity nor opioid consumption was noted. No significant side effects were observed.
Machoki et al.'s92 study with adequate baseline analgesia compared continuous wound instillation to epidural analgesia using an infusion pump, both containing 0.2% bupivacaine at a rate of 0.1 to 0.2 ml kg−1 h−1, to a third group receiving standard postoperative analgesia. In the group receiving wound instillation, a clinically significant reduction of average pain scores, as well as significantly reduced morphine consumption, was demonstrated compared with the two other groups. No adverse effects were reported.
Open appendicectomy: mixed populationRandall et al.’ randomised clinical trial with a mixed population investigated the difference between preoperative local subcutaneous infiltration versus subcutaneous and deep to external oblique infiltration with 2 mg kg−1 bupivacaine.93 Both groups showed low postoperative pain scores, although the group with deep infiltration had a clinically and statistically significant pain reduction at 24 h. Adequate baseline analgesia was utilised, and no opioid-sparing effect was reported.
KetamineOne study94 in adults and one95 in a paediatric population, including 155 patients, investigated the effect of preoperative systemic ketamine in patients undergoing open appendicectomy. Behdad et al.94 compared the intravenous application of 0.5 mg kg−1 of ketamine 10 min preoperatively compared with saline in adults. The VAS score was significantly reduced by ketamine application for 24 h postoperatively without opioid-sparing effect and without reporting adequate baseline analgesia. Dix et al.95 compared the effect of ketamine in children undergoing open appendicectomy in a three-arm trial. One group received a preoperative intravenous ketamine bolus (500 μg kg−1), the next group received, in addition to the ketamine bolus, a ketamine infusion (4 μg kg−1 min−1) postoperatively, and the last solely received a 0.9% saline infusion as the control group. The pain scores in all three groups showed no difference, as well as opioid consumption. The request for additional NSAIDs was significantly higher in the ketamine infusion group. Furthermore, the side effects in the form of headaches were higher in the ketamine infusion group.
Other therapiesTwo studies (212 patients) investigated the effect of peritoneal closure to nonclosure. One concerning the adult population showed no difference, and the other regarding children with a significant reduction in pain with lower analgesic consumption in the nonclosure group.96,97
Two studies by Kleif et al.98,99 studied the effects of 8 mg intravenous dexamethasone and 125 mg intravenous methylprednisolone approximately 30 min before surgery compared with placebo in adults. On the first postoperative day, a significantly reduced VAS score and morphine-sparing effect could be demonstrated in the dexamethasone group. The methylprednisolone group showed no significant difference. Routine analgesia was administered but not specified in the dexamethasone study and reported adequately in the methylprednisolone study.
One study compared general to combined spinal/epidural anaesthesia with bupivacaine and fentanyl in adults. There was a significantly reduced VAS score lasting 24 h postoperatively in the spinal/epidural group with the opioid-sparing effect with the exception at 6 h.100 Baseline analgesia was not reported, and except for shoulder pain, more side effects were associated with the combined spinal/epidural method.
Lau et al.101 examined the efficacy of needlescopic appendicectomy using smaller ports and instruments compared with conventional laparoscopic appendicectomy. The intervention showed no difference in analgesic outcome with a higher conversion rate and longer operative time.
A study of 60 adult patients compared conventional laparoscopic appendicectomy to a double-incision, three-port approach.102 Except for a significantly improved cosmetic outcome, no differences in pain intensity were reported.
Lee et al.103 compared the use of a patch containing 175 mg lidocaine applied periumbilically after laparoscopic appendicectomy to a patch without active ingredients. The reported VAS scores did not report differences, but the pethidine consumption was significantly reduced in the lidocaine group. Neither was adequate baseline analgesia reported nor adverse effects attributed to the lidocaine patch.
Hamill et al. demonstrated a time-limited but clinically significant pain reduction by performing a rectus sheath block with 0.25% bupivacaine compared with a placebo in children.104 Adequate baseline analgesia was utilised, but no opioid-sparing effect was noticed.
Two studies with adequate baseline analgesia investigated different methods regarding insufflation during laparoscopic appendicectomies in children.105,106
Yu et al.105 compared warm humidified carbon dioxide insufflation to standard insufflation, and Baird et al.106 compared nebulization of 0.5% ropivacaine at the onset of surgery to 0.9% saline nebulisation. Both studies reported no difference in pain intensity or opioid consumption.
Sola et al.107 compared standard PCA with morphine or hydromorphone combined with intravenous ketorolac (0.5 mg kg−1 6 hourly) to the same analgesia with the addition of intravenous paracetamol (10 mg kg−1 6 hourly) in children with perforated appendicitis undergoing laparoscopic appendicectomy. No analgesic benefit or improved opioid consumption was reported.
Jangjoo et al.'s randomised trial demonstrated significantly reduced pain scores and opioid consumption while comparing preoperative rectal indomethacin (100 mg) application versus placebo in adult patients undergoing open appendicectomies.108 The use of adequate baseline analgesia was not described.
Nazemi's109 trial showed a clinically relevant reduction in pain intensity at rest and while coughing using 10 mg kg−1 of pentoxifylline preoperatively in adult patients undergoing laparoscopic appendicectomy. A significantly lower analgesic consumption and no complications attributed to pentoxifylline were reported.
Eskandarlou et al.110 compared a new right groin incision to the conventional McBurney's incision in adults showing a significantly increased pain intensity in the intervention group.
A single trial by Okereke et al.111 investigated the effect of skin incision by diathermy or scalpel in adults subject to open appendicectomy. There was a higher mean pain intensity in the diathermy group but without significance. Adequate baseline analgesia and no adverse effects were reported.
Two studies112,113 including 280 patients undergoing open appendicectomies, investigated the effect of suture methods in a mixed population. Both compared subcuticular to transdermal sutures. Malekpour Alamdari et al.112 showed no difference, whereas Javadi et al.113 reported a significantly reduced pain score on postoperative day 7 for the subcuticular sutures. Neither of them displayed adequate baseline analgesia nor reported analgesic consumption.
A three-arm trial by Gazerani et al.114 compared the effect of aromatherapy with geranium and almond oil to no intervention, showing a clinically reduced pain intensity in both groups receiving aromatherapy. No adequate baseline analgesia was reported.
One study compared the appendix stump's closure with Hem-o-lok clips to intracorporeal knotting in adults during laparoscopic appendicectomy, showing no significant difference in pain outcome.115
DiscussionPain intensity after appendicectomy is underestimated and not well managed in clinical practice.5 Therefore, an evidence-based recommendation of best treatment options with a balanced efficacy-risk is highly needed. We found a high number of studies to be included in this systematic review and PROSPECT recommendation. The data of adults and children were combined as there were no differences in surgical or anaesthetic techniques. The children participating in the studies were capable of using pain intensity rating scales. On the basis of the available evidence and the PROSPECT methodology,14 several recommendations could be formulated as compiled in Table 1. These recommendations differ between laparoscopic versus open appendicectomy. A considerable number of analgesic techniques are not recommended simply because of limited or lack of evidence (Table 2). It does not mean that these techniques and drugs (e.g. systemic co-analgesics) are ineffective; in many cases, there is just insufficient data available to consider a clear recommendation.
Table 1 - Recommendations for procedure-specific pain management in patients undergoing appendicectomy for adults and children Overall recommendations: surgical aspects Three-port laparoscopic surgery is recommended over open appendicectomy (grade A) Laparoscopic appendicectomy Preoperative and intra-operative Intraperitoneal local anaesthetics (grade A) Postoperative Systemic analgesia should include paracetamol and NSAID (or COX-2-selective inhibitor in adults) administered preoperatively or intra-operatively and continued postoperatively for basic analgesia as for other procedures (grade A) Opioid for rescue medication (grade D) Open appendicectomy Pre and intra-operative TAP block (grade A) Preincisional infiltration with local anaesthetics into skin and external oblique (Grade A), if TAP block is not possible Postoperative Systemic analgesia should include paracetamol and NSAID (or COX-2-selective inhibitor in adults) administered preoperatively or intra-operatively and continued postoperatively for basic analgesia as for other procedures (grade A) Opioid for rescue medication (grade D)
留言 (0)