
記住我
Clinical trials are crucial to the advancement of products and procedures related to the shoulder and elbow. The Food and Drug Administration Modernization Act of 1997 required the United States Department of Health and Human Services, acting through the National Institutes of Health (NIH), to establish a registry of clinical trials information for both federally and privately funded trials, resulting in the creation of ClinicalTrials.gov.1,2 This is an Internet-based registry and results database that became publicly available in February 2000.
Registration and results data are reported to ClinicalTrials.gov by sponsors and investigators, and the database is maintained by the NIH through the National Library of Medicine.1 Registration data cataloged by ClinicalTrials.gov include trial characteristics, such as the intervention type under active investigation, phase, randomization, and blinding.
Previous studies analyzing clinical trials registered with ClinicalTrials.gov have focused on publication rates and factors related to publication of trial results, as well as the rates, reasons, and predictors of trial termination.3–5 However, sponsorship trends have not been specifically evaluated for clinical trials related to the shoulder and elbow, nor have trial characteristics been compared among shoulder and elbow trials sponsored by institutions, industries, and federal agencies.
This study sought to characterize the types and trends of sponsorship for shoulder and elbow clinical trials. Furthermore, this study sought to compare trial characteristics among trials sponsored by institutions, industries, and federal agencies.
Methods Study SampleThe ClinicalTrials.gov database was queried on January 12, 2023, for clinical trials from the launch of ClinicalTrials.gov (February 29, 2000) through December 31, 2022, using the search terms ‘shoulder’ and ‘elbow.’ Use of these data was deemed exempt from review by our Institutional Review Board.
Trial CharacteristicsTrial characteristics were abstracted from ClinicalTrials.gov as categorical variables. Some were grouped to facilitate interpretation, and definitions are provided below. Trial characteristics were abstracted, including start year, the type of intervention actively under investigation (eg, procedure, device, drug, biological product, and other), phase, randomization, and blinding.
ClinicalTrials.gov defines the trial sponsor as ‘the organization or person who initiates the study and who has authority and control over the study.’5 Categories of study sponsorship were federal (ie, sponsorship by the NIH or another US federal agency), industrial, and institutional, the latter of which this study defined as including sponsorship by individuals, universities, and community-based organizations.
Trial intervention is defined according to the ‘process or action that is the focus of a clinical study.’6 Intervention types were categorized as procedure, device, biological product, drug, behavioral, or other. Other included the following intervention types: combination product, diagnostic testing, dietary supplementation, genetic, radiation, and other.
The phases of study captured the study design. Phase I captured what was included in the data set as early phase I and phase I studies. Phase II captured what was included in the data set as phase II and I/II studies. Phase III captured what was included in the data set as phase III and II/III studies. For some studies, this was not applicable (N/A).
Studies were also characterized as randomized (ie, yes or no) and blinded (ie, yes or no). Blinding was abstracted as a dichotomous variable to indicate whether the participant, care provider, investigator, and/or outcomes assessor was blinded.
Data AnalysesUnivariate χ2 analyses were performed for shoulder and elbow clinical trials to compare the distribution of trial characteristics among trials sponsored by federal agencies, industry, and institutions. Pairwise multivariate logistic regressions were used to determine associations between institutional versus industrial or federal sponsorship and other trial characteristics.
Statistical analyses were performed with RStudio.7 Significance was set to 0.05. Forest plots were generated in Microsoft Excel8 and used to present the results of multivariate analyses.
Results Sponsorship TrendsA total of 4,945 shoulder clinical trials and 1,517 elbow clinical trials were identified, of which 26 shoulder clinical trials and seven elbow clinical trials were excluded due to incomplete reporting of trial registration data. Of the 4,919 shoulder trials included in the study sample, institutions sponsored 4,342 trials (88.3%), industries sponsored 509 trials (10.3%), and federal agencies sponsored 68 trials (1.4%). Of the 1,510 elbow trials included in the study sample, institutions sponsored 1,303 trials (86.3%), industries sponsored 186 trials (12.3%), and federal agencies sponsored 21 trials (1.4%).
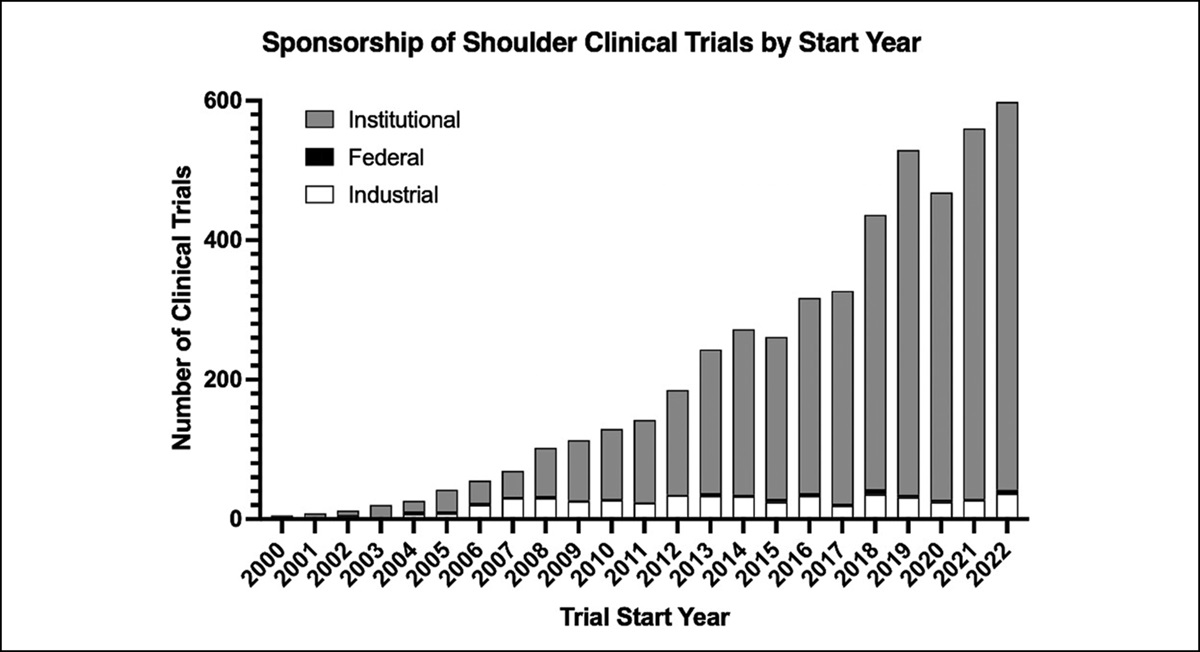
From 2000 to 2022, the number of shoulder trials initiated annually markedly increased (from 5 to 598, representing an increase of 59,700%). Over the same period, the number of elbow trials initiated annually markedly increased (from 2 to 236, representing an increase of 23,500%). This was predominantly driven by an increase in the number of institutionally sponsored trials (Figures 1 and 2). In 2000, institutions initiated one shoulder trial and one elbow trial, whereas in 2022, institutions initiated 556 shoulder trials and 236 elbow trials (increase by 55,500% and 21,400%, respectively).
 Figure 1:
Figure 1: Chart illustrating the sponsorship of shoulder clinical trials started from February 29, 2000, to December 31, 2022.
 Figure 2:
Figure 2: Chart illustrating the sponsorship of elbow clinical trials started from February 29, 2000, to December 31, 2022.
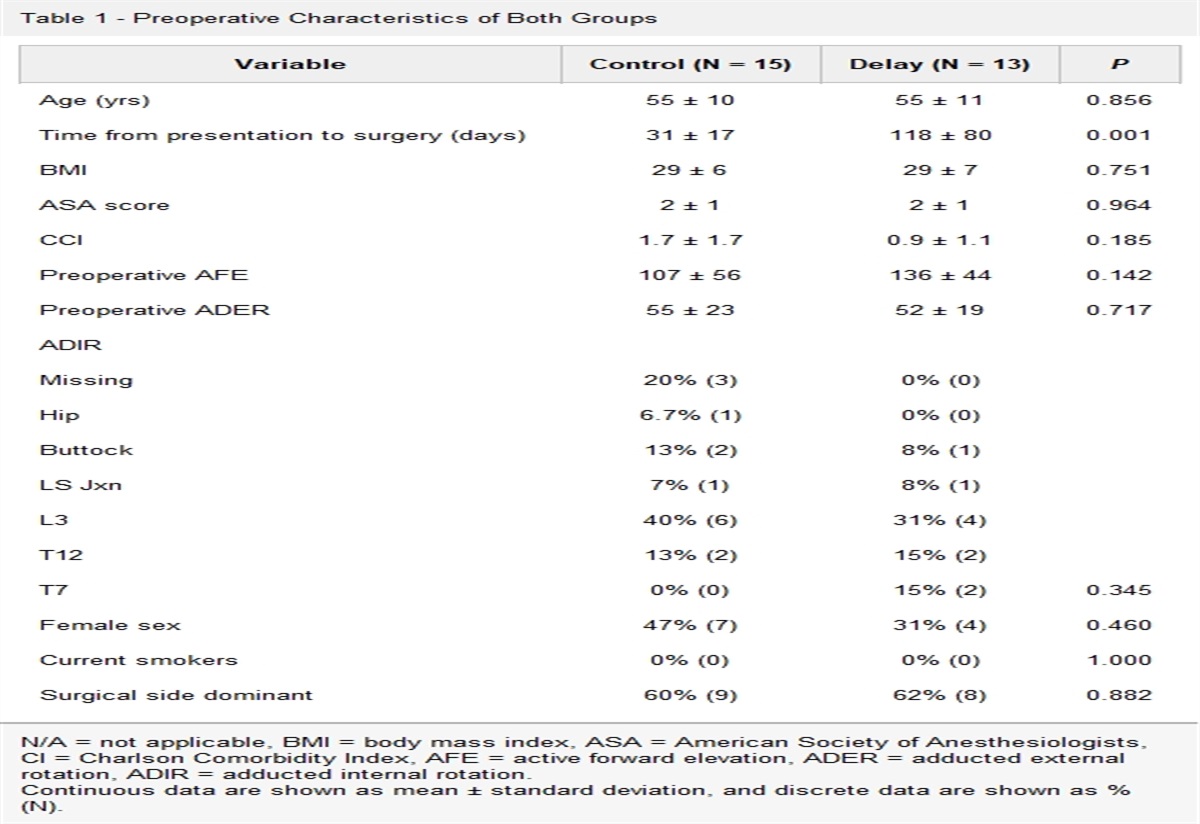
Association of Trial Characteristics with Sponsorship TypesTrial characteristics for shoulder and elbow clinical trials are summarized in Tables 1 and 2, respectively. On univariate analysis of the study sample, all trial characteristics assessed (intervention type, phase, randomization, and blinding) were found to be correlated with sponsorship type (P < 0.05 for each).
Table 1 - Shoulder Clinical Trials: Univariate Chi-Square Analysis for Trial Characteristics Distributed Among Clinical Trials Related to the Shoulder Sponsored by Institutions, Industry, and Federal Agencies Sponsorship: N (%) P Institutional Industrial Federal Total trials = 4919 4342 (88.3%)a 509 (10.3%)a 66 (1.4%)a — Intervention type Procedure 869 (20.0%) 14 (2.8%) 14 (20.6%) 0.000 Device 659 (15.2%) 148 (29.1%) 22 (32.4%) Biological 53 (1.2%) 66 (13.0%) 2 (2.9%) Drug 568 (13.1%) 262 (51.5%) 14 (20.6%) Behavioral 431 (9.9%) 1 (0.2%) 8 (11.8%) Other 1762 (40.6%) 18 (3.5%) 8 (11.8%) Phase I 91 (2.1%) 32 (6.3%) 1 (1.5%) 0.000 II 183 (4.2%) 124 (24.4%) 10 (14.7%) III 165 (3.8%) 148 (29.1%) 3 (4.4%) IV 286 (6.6%) 40 (7.9%) 6 (8.8%) N/A 3617 (83.3%) 165 (32.4%) 48 (70.6%) Randomized? Yes 3597 (82.8%) 327 (64.2%) 55 (80.9%) 0.000 No 745 (17.2%) 182 (35.8%) 13 (19.1%) Blinded? Yes 2790 (64.3%) 263 (51.7%) 42 (61.8%) 0.000 No 1552 (35.7%) 246 (48.3%) 26 (38.2%)CI = confidence interval.
aPercentage values accompanied. Reflect the percentage of the total clinical trials in the study sample (N = 4,919 trials).
Boldface indicates statistical significance (p<0.05).
CI = confidence interval.
aPercentage values accompanied by asterisk. Reflect the percentage of the total clinical trials in the study sample (N = 1,510 trials).
Boldface indicates statistical significance (p<0.05).
Multivariate analyses were performed to evaluate whether trial characteristics were independently associated with sponsorship types. To do this, trial characteristics were compared first among trials sponsored by industry relative to institutionally sponsored trials and then among trials sponsored by federal agencies relative to institutionally sponsored trials (Table 3 for shoulder trials and Table 4 for elbow trials).
Table 3 - Results of Pairwise Multivariate Analyses for Trial Characteristics Among Shoulder-Related Clinical Trials With Industrial, Institutional, and Federal Sponsorship Sponsorship Institutional [ref.] Industrial Federal OR (95% CI) P OR (95% CI) P Intervention type Procedure [ref.] — 1.00 — 1.00 — Biological — 27.66 (14.19, 56.9) <0.0001 1.78 (0.26,7.30) 0.4767 Device — 15.41 (8.99, 28.55) <0.0001 2.12 (1.08, 4.29) 0.0315 Drug — 14.22 (8.18, 26.60) <0.0001 1.19 (0.50, 2.85) 0.6916 Behavioral — 0.16 (0.01, 0.79) 0.0748 1.19 (0.47, 2.82) 0.6938 Other — 0.80 (0.39, 1.66) 0.5372 0.30 (0.12, 0.71) 0.0073 Phase I [ref.] — 1.00 — 1.00 — II — 2.12 (1.26, 3.61) 0.0052 4.99 (0.91, 93.41) 0.1324 III — 3.16 (1.88, 5.40) <0.0001 1.76 (0.21, 36.70) 0.6306 IV — 0.37 (0.21, 0.66) 0.0007 1.93 (0.31, 37.61) 0.5535 Not applicable — 0.35 (0.20, 0.59) <0.0001 1.60 (0.32, 29.32) 0.6497 Randomized? Yes [ref.] — 1.00 — 1.00 — No — 2.31 (1.67, 3.19) <0.0001 1.01 (0.48, 2.04) 0.9743 Blinded? Yes [ref.] — 1.00 — 1.00 — No — 1.44 (1.06, 1.93) 0.0178 1.07 (0.59, 1.89) 0.8103CI = confidence interval, OR = odds ratio, ref. = reference.
Boldface indicates statistical significance (p<0.05).
CI = confidence interval; ref. = reference.
aToo few trials to calculate odds ratio (OR).
Boldface indicates statistical significance (p<0.05).
Relative to shoulder clinical trials with institutional sponsorship, industry sponsorship was independently associated with intervention type (relative to procedure studies, studies related to biological products odds ratio [OR] = 27.66, devices OR = 15.41, and drugs OR = 14.22), phase of study (relative to phase I, phase II OR = 2.12, phase III OR = 3.16, phase IV OR = 0.37, and not applicable OR = 0.35), nonrandomized trials OR = 2.31, and trials without blinding OR = 1.44 (P < 0.05 for each). That is, industry-sponsored shoulder trials were more likely to be investigating biological products, devices, and drugs; phase II or III; not to be randomized; and lack blinding relative to shoulder trials sponsored by institutions. Industry-sponsored shoulder trials were also less likely to be phase IV and not have a phase (ie, phase not applicable) when compared with institutionally sponsored shoulder trials.
Relative to shoulder clinical trials with institutional sponsorship, federal sponsorship was independently associated with intervention type (relative to procedure studies, studies related to devices OR = 2.12 and other OR = 0.30; P < 0.05 for each). That is, federally sponsored shoulder trials were more likely to be investigating devices and less likely to be trialing other investigational products relative to shoulder trials sponsored by institutions.
Relative to elbow clinical trials with institutional sponsorship, industry sponsorship was independently associated with intervention type (relative to procedure studies, studies related to biological products OR = 67.17, drugs OR = 64.31, and devices OR = 33.20), phase of study (relative to phase I, phase III OR = 4.01, phase IV OR = 0.18, and not applicable OR = 0.19), and nonrandomized OR = 5.15 (P < 0.05 for each). That is, industry-sponsored elbow trials were more likely to be investigating biological products, drugs, and devices; phase III; and not to be randomized. Industry-sponsored elbow trials were also less likely to be phase IV and not have a phase when compared with institutionally sponsored elbow trials. Relative to elbow trials with institutional sponsorship, federal sponsorship was not associated with intervention types, phase of study, randomization, and blinding.
DiscussionClinical trials are critical to the advancement of science and technologies in all clinical areas, including those related to the shoulder and elbow. This is a cross-sectional study of shoulder and elbow clinical trials registered with ClinicalTrials.gov that found the number of shoulder and elbow clinical trials initiated annually increased markedly between 2000 and 2022, largely driven by an increase in institutionally sponsored clinical trials for trials related to the shoulder and elbow.
This change in sponsorship trends over the years is likely multifactorial. It is widely acknowledged that federal grants have become incrementally harder to secure over the years.9–11 Furthermore, industry might have become more hesitant to support trials, especially in light of reasons leading to trial termination in areas such as spine4 and shoulder/elbow5; most commonly, sponsors and investigators for these trials report difficulties in subject accrual and/or retention, business decision and/or strategic reasons (eg, restructuring of organizations and focusing on different business/strategic initiatives), and issues related to regulatory and compliance in the conduct of the clinical trial. Only in a minority of clinical trials were trials terminated due to scientific data emerging from the trial itself (eg, lack of efficacy of the investigational product). Alternatively, it is also possible that there are now fewer barriers and/or more local sources of support available for initiation of clinical trials by institutions; the impact of such support for institution-led research has been documented in other research areas; examples of these sources of support include federal grants, institutional grants from in-house funding, and support provided to institutions from collaboration with industry.12–15
When the registration characteristics were compared among shoulder and elbow clinical trials sponsored by industry, institutions, and federal agencies, all trial characteristics (intervention type, phase, randomization, and blinding) were correlated with sponsor type; that is, univariate analysis revealed differences in the types of studies initiated by industry, institutions, and federal agencies. To investigate more rigorously whether trial characteristics would be independently associated with sponsorship types, multivariate analysis was performed with trials sponsored by federal agencies and industry compared in a pairwise manner with institutionally sponsored trials.
Relative to shoulder clinical trials with institutional sponsorship, industry sponsorship was independently associated with intervention type, phase, nonrandomized trials, and trials without blinding. Relative to shoulder clinical trials with institutional sponsorship, federal sponsorship was independently associated with intervention type only. For example, with procedure as the reference for trial intervention type, shoulder-related trials sponsored by industry were more likely to investigate devices, biological agents, and drugs relative to those sponsored by institutional trials. Differences in trial design characteristics may help to explain prior findings by Caruana et al4 that clinical trials sponsored by industry are more likely to result in termination relative to those sponsored by institutions.. What this work adds to the literature is an understanding of how different clinical trial design characteristics are linked to sponsorship type. Increased attention to the challenges faced by industry sponsors, as well as policies to support device-, biological-, and drug-related clinical trials, may help industry sponsors avoid trial termination, ultimately facilitating the advancement of new products and procedures for diseases and disorders of the shoulder.
Relative to elbow clinical trials with institutional sponsorship, industry sponsorship was independently associated with intervention type, phase of study, nonrandomized, and trials with blinding. As with clinical trials of the shoulder, increased attention to the challenges faced by industry sponsors, as well as policies to support device-related clinical trials, may help industry sponsors avoid trial termination, ultimately facilitating the advancement of new products and procedures for diseases and disorders of the elbow. We must provide caution, however, noting that industry-sponsored shoulder trials were more likely to lack randomization and blinding, and industry-sponsored elbow trials were more likely to lack randomization, and furthermore, industry-sponsored spine-related clinical trials were found to report positive outcomes at a higher rate, potentially reflecting bias in study design.18 The authors would urge industry sponsors to use blinding and randomization whenever is possible so as to limit bias in reporting of results, especially if additional support is to be provided to industry to avoid trial termination.
There are several limitations to this study. Cross-sectional sampling of trials registered at ClinicalTrials.gov limits data collection to a single time point (ie, January 12, 2023—the date the ClinicalTrials.gov database was queried) and to ‘applicable clinical trials’ defined by the Final Rule for Clinical Trials Registration and Results Information Submission (ie, generally, phase II through IV trials investigating FDA-regulated interventions that are conducted in the United States).17 There are likely to be clinical trials advancing science and technologies related to conditions of the shoulder and elbow that were registered with ClinicalTrials.gov in addition to those captured in the study sample but that did not include the terms ‘shoulder’ or ‘elbow’ in any of the following trial registration data elements and, thus, were not captured: title, condition/disease, or intervention(s). Therefore, this study likely captures only a subset of clinical trials related to the shoulder and elbow and, thus, underestimates the true number of clinical trials related to interventions under active investigation for diseases and disorders of the shoulder and elbow. Registration of clinical trials with the NIH was not required until 1997 by the Food and Drug Administration Modernization Act and ClinicalTrials.gov was not made publicly available until February 29, 2000.1 Furthermore, to facilitate analysis, some terms were combined as defined in the methods of the paper, but this could have affected the granularity of some of the data assessed. For example, blinding was treated as a dichotomous variable (ie, studies that used blinding at any level and studies lacked blinding entirely); although this simplified data classification for the purposes of logistic regression, the nuance that accompanies consideration of blinding in its many forms (eg, blinding of the investigators, statisticians, clinical teams, and/or subjects) was not considered here.
In summary, the number of shoulder and elbow clinical trials initiated annually markedly increased between 2000 and 2022, driven by an increase in institutionally sponsored trials. For clinical trials related to the shoulder, design characteristics were found to differ based on study sponsorship type (industrial and federal relative to institutional). Given the disproportionate increase in institutionally sponsored trials, this suggests that the design characteristics of shoulder-related clinical trials are shifting over time.
AcknowledgmentsThe authors acknowledge that this work would not have been possible without the ongoing efforts by the National Library of Medicine in collecting trial registration data from sponsors/investigators and in maintaining the ClincialTrials.gov database.
References 1. U.S. National Library of Medicine. ClinicalTrials.gov background. 2021. Accessed February 28, 2023. 2. U.S. National Library of Medicine. History, Policies, and Laws. ClinicalTrials.gov. 2023. Accessed February 28, 2023. 3. Ohnmeiss DD: The fate of prospective spine studies registered onwww.ClinicalTrials.gov. Spine J 2015;15:487-491. 4. Caruana DL, Nam-Woo Kim D, Galivanche AR, et al.: Analysis of the frequency, characteristics, and reasons for termination of spine-related clinical trials. Clin Spine Surg 2022;35:e596-e600. 5. Caruana DL, Gouzoulis MJ, McLaughlin WM, Grauer JN: Analysis of the frequency, characteristics, and reasons for termination of shoulder- and elbow-related clinical trials. J Shoulder Elbow Surg 2022;31:1922-1928. 6. U.S. National Library of Medicine. Glossary of common site terms. ClinicalTrials.gov. 2021. Accessed February 28, 2023. 7. R Foundation for Statistical Computing. R Statistical Programming. Version 4.2.2. 2021. 8. Microsoft Corporation. Microsoft® Excel for Mac
留言 (0)