
記住我
Subacute combined degeneration (SCD) of the spinal cord is a disease involving the lateral and posterior columns of the spinal cord. It can manifest in patients with known or subclinical vitamin B12 deficiency and cause hematologic and neurologic disruptions.1 Vitamin B12 deficiency can result from decreased intake or absorption, and it can also be caused by certain medications such as proton-pump inhibitors and metformin as well as nitrous oxide.2
Nitrous oxide (N2O) otherwise known as laughing gas has been used clinically as an anesthetic for more than 150 years.3 Along with its analgesic properties, it can also cause dizziness, euphoria, derealization, and depersonalization when inhaled.4 Cases of neurologic damage from N2O use have been described in the literature, and it is now known that N2O interferes with the metabolism of vitamin B12. N2O oxidizes the cobalt ion of vitamin B12 and inhibits its ability to act as a coenzyme; this ultimately results in unstable myelin sheaths and subsequent demyelination in the central and peripheral nervous systems.5
N2O-induced SCD of the spinal cord was first described in 1978 when several dentists were abusing nitrous oxide and developed neurologic symptoms.6 Until recently, the literature on this topic was largely focused on N2O-induced SCD of the spinal cord as an infrequent complication of N2O anesthesia. This would particularly occur in patients with preexisting vitamin B12 deficiencies.7 Over the last decade or so, recreational N2O use has markedly increased and with it N2O-induced SCD has risen as well. N2O was reported as the seventh most used recreational drug in the 2016 Global Drug Survey and is commonly available to the public as an aerosol spray propellant in the food industry.4,8 It has been reported that 3.4% of N2O recreational users experience neurologic symptoms, although this may be an underestimate as reports of N2O-induced SCD cases continue to rise.7
N2O-induced SCD is commonly misdiagnosed, and therefore, it is often inappropriately treated. Given the nature of the neurologic deficits many of these patients experience, spine surgeons may encounter these patients in the clinic or be consulted to evaluate these patients in the hospital setting. Awareness in the spine surgery community is important to reduce the risk of long term, possibly irreversible neurologic damage by ensuring accurate diagnosis and treatment. Given wide availability of N2O, clinicians must maintain a high index of suspicion when confronting patients with concerning clinical pictures.
Illustrative CaseInformed consent was obtained from the patient for the use of this information for submission and publication. A 44-year-old woman presented to our spine surgery clinic with a 3-week history of progressive bilateral upper and lower extremity weakness with associated paresthesias of unknown origin. Her medical history included previous gastric bypass, attention deficit disorder, anxiety disorder, bipolar disorder, history of substance abuse, and depression. She developed severe nausea and vomiting 3 days after her use, prompting an evaluation in the emergency department. She was admitted for medical management and was deemed stable and discharged 3 days later. Of note, she did have a complete blood count laboratory test indicative of megaloblastic anemia at this time. The patient reported that 2 to 3 days after discharge she noted “tingling” to the plantar aspect of her left foot. The paresthesias about her left foot slowly progressed proximally and soon began to involve her right lower extremity as well. This led to progressive leg weakness and gait disturbance leading to multiple falls at home. In addition, the patient reported paresthesias and weakness to her bilateral upper extremities, and she began having difficulty with hand dexterity. She did not have any neck or back pain and was without radicular symptoms. No recent trauma or illness was found. She had no bladder or bowel dysfunction, and the remainder of her review of systems was negative.
On initial physical examination, her integument was intact without lesions, rashes, or evidence of trauma. Her spine and back were largely nontender. She had global weakness and decreased sensation to light touch about her bilateral lower extremities in a nondermatomal distribution. Proximal muscle groups to upper and lower extremities had muscle gradings of 3s and 4s of 5. Weakness was most pronounced distally about both upper and lower extremities. Ankle and great toe dorsiflexion, wrist extension, and hand intrinsics were the weakest, with muscle gradings of 1s and 2s of 5. Her gait was ataxic. Sensation about the bilateral upper extremities was also globally decreased to light touch, and she had marked weakness about bilateral wrist extension. She had a normal vascular examination about the bilateral lower and upper extremities, and provocative testing including bilateral straight leg raise and spurling's were negative.
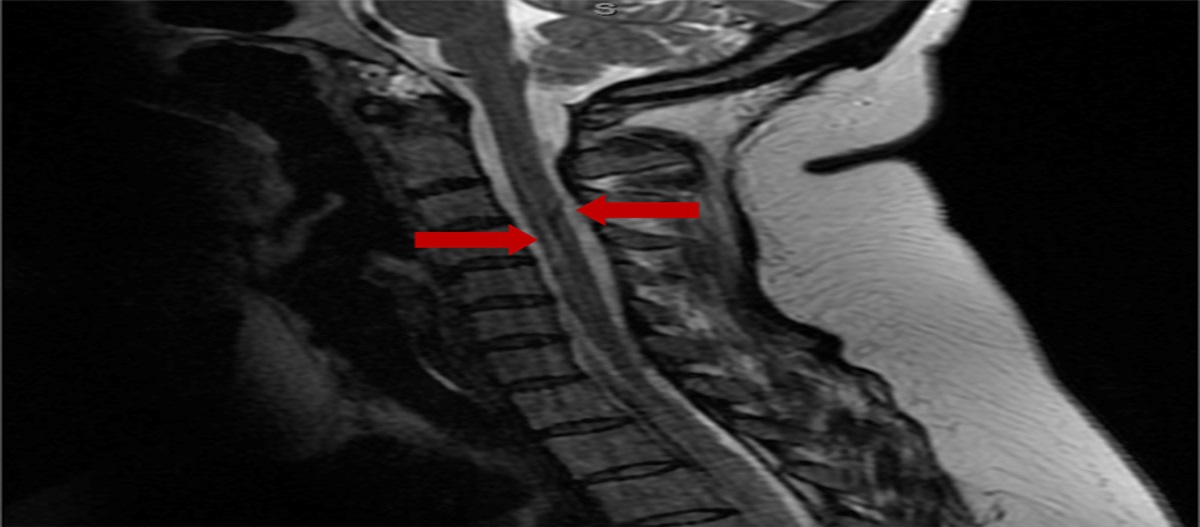
The clinical picture was initially clouded; however, after further history taking, the patient hesitantly reported that she was huffing nitrous oxide gas through balloons and other mechanisms for “several hours” three and half weeks prior. She was sent to the emergency department for additional evaluation and work-up. MRI and CT scans of her brain, cervical, thoracic, and lumbar spine were obtained and were negative for acute processes, which would explain the patient's neurologic symptoms. MRI did however show abnormal hyperintense signals about the dorsal and lateral spinal cord (Figures 1 and 2). The possibility of nitrous oxide poisoning promoted specific laboratory tests to be ordered. Laboratory results included a low vitamin B12 level of 146 pg/mL (normal 270 to 1,000 pg/mL), an elevated homocysteine level of greater than 50 μmol/L (normal 4 to 10 μmol/L), and an elevated methylmalonic acid level of 1.87 nmol/mL (normal <0.4 nmol/mL). Her folate level was normal at 6.7 ng/mL (normal >5.4 ng/mL). Toxicology screen of the urine was done, which was positive only for benzodiazepines. An ECG was done revealing normal sinus rhythm. A lumbar puncture was done, and cerebrospinal fluid was with normal glucose and protein levels, no RBCs or nucleated cells, and cultures were negative.
 Figure 1:
Figure 1: Sagittal MRI image of the cervical spine with abnormal hyperintense signal about the dorsal and lateral spinal cord as identified by arrows.
 Figure 2:
Figure 2: Axial MRI image of the cervical spine at the C2-3 level with abnormal hyperintense signal about the dorsal and lateral spinal cord as identified by the arrows.
The patient was initially treated with vitamin B12 supplementation at a dose of 1,000 mcg intramuscular (IM) daily, and symptoms began to slowly improve. After 4 days, she was discharged home with this daily IM vitamin B12 supplementation dose and plans for follow-up with internal medicine, neurology, and physical medicine and rehabilitation. She initially used a wheelchair for ambulation and had in-home therapy for 2 weeks until transitioning to outpatient occupational and physical therapy. At 3-week follow-up, she had achieved above normal vitamin B12 levels >2,000 pg/mL and supplementation was decreased to one 1,000 mcg IM injection per week. At 6-week follow-up, she continued to improve about her motor function and her vitamin B12 supplementation dose was decreased to one 1,000 mcg IM injection per month. At 3-month follow-up, she had transitioned from a wheelchair to a rollator walker with the use of bilateral ankle foot orthosis for ambulation. She remained with bilateral wrist and foot drop and notable intrinsic hand atrophy and weakness. At 6-month follow-up, she remained in outpatient physical and occupational therapy and was weaning from her walker. She was taking Lyrica for residual neuropathic pain, and her motor and sensory symptoms continued to show improvement with motor grades of 4s and 5s about her proximal upper and lower extremities. She did remain with notable weakness to ankle dorsiflexion, wrist extension, and intrinsic hand musculature bilaterally. Her sensation improved to light touch about bilateral upper and lower extremities and however remained decreased to pinwheel throughout. A detailed timeline is given in Table 1.
Table 1 - Detailed Timeline of the Patient's Clinical Course and Follow-up Timeline Day 1 Week 1 Week 3 Week 6 Week 12 Week 18 Week 30 Event Date of N2O abuse ED visit Spine surgery clinic and hospital admission 1st follow-up 2nd follow-up 3rd follow-up 4th follow-up Clinical course Nausea/vomiting, lower extremity paresthesias with progressive leg weakness Muscle gradings of 3s and 4s proximally and 1s and 2s distally with decreased sensation about bilateral upper and lower extremities Normal vitamin B12 levels achieved, continued marked weakness Proximal musculature to upper and lower extremities showing improvement Transition from wheelchair to walker using bilateral AFOs Weaning from walker, muscle gradings of 4s and 5s proximal upper and lower extremities with 1s and 2s to ankle dorsiflexion, wrist extension, and intrinsic hand musculature bilaterallyPatients affected by nitrous oxide–induced SCD of the spinal cord are typically younger, aged between 16 and 30 years with a 75% male predominance. It is known that the risk of developing SCD is greater with increased N2O use and most patients presenting to an acute care setting have had long-term recreational use.7 A notable amount of recreational N2O use is through the use of whipped cream canisters where N2O is found as an aerosol spray propellant. Pressurized whip cream chargers, otherwise known as “whippets,” can also be attached to a balloon which enables another method of gas inhalation. Effects after inhalation may include euphoria, distortions of sound, and mild hallucination; these are short acting and typically resolve in just a few minutes. The quick-on and quick-off effects of N2O may prompt users to continue with frequent repeated inhalation. Some common adverse effects after subsidence of psychotropic effects include nausea and vomiting, headaches, and blurred vision.8
Prolonged N2O use leads to interference of the vitamin B12 metabolic pathway. N2O irreversibly oxidizes the cobalt ions of vitamin B12 inactivating it, therefore leaving it unavailable to act as a coenzyme to convert both homocysteine to methionine and methyl-malonyl-coenzyme A to succinyl coenzyme A. Serum homocysteine levels are then increased, and the methylation of myelin proteins is interrupted, which causes unstable myelin sheaths and ultimate demyelination in the central and peripheral nervous systems.5 Neurologic dysfunctions in vitamin B12 deficiency typically affect the spinal cord first and many times exclusively. The process usually begins in the posterior columns and spreads to the lateral and anterior columns. Demyelination can be seen on T2-weighted MRI images as high-intensity lesion.9 Symptoms of N2O-induced SCD can present over a variable timeline from days to months as is seen in classic SCD as well. Initially, patients will often note distal paresthesias about their limbs in their hands and feet. Symptoms may progress to gait imbalance, difficulty with ambulation and even. Weakness, Lhermitte phenomenon, bladder or bowel urgency or incontinence, sexual dysfunction, or psychiatric symptoms may also be seen. Examination findings are often symmetrical including posterior column symptoms such as loss of vibration and proprioception. Both hyperreflexia and hyporeflexia are possible as is an extensor plantar response.7
LessonsPatients with underlying subclinical vitamin B12 deficiency can be affected at lower doses of both recreational and anesthetic N2O; therefore, clinicians should inquire about risk factors.7,10,11 Although the diagnosis is clinical, a detailed history and physical examination are pertinent. The diagnosis should be supported by various hematologic, neurologic, and imaging findings, and other diagnoses on the differential must be investigated. Pernicious anemia is the most common cause of vitamin B12 deficiency, and other possible causes including certain medications, diets, pancreatic or small bowel lesions, previous small bowel or gastric procedures, and Crohn's disease should be investigated.7 Copper and vitamin E deficiency may also mimic SCD symptoms from vitamin B12 deficiency and should be ruled out as well.12,13 Metformin and acid-suppressing medications such as histamine receptor antagonists and proton pump inhibitors have also been linked to vitamin B12 deficiency.2 Patients undergoing bariatric surgery procedures such as Roux-en-Y gastric bypass and gastric sleeve are at high risk for vitamin B12 deficiency. These patients subsequently produce less gastric acid preventing full breakdown of food-bound vitamins, intrinsic factor is reduced or absent, vitamin B12 malabsorption can occur, and a general reduction in food intake perioperatively can have a negative effect as well.5
When a clinical diagnosis of N2O-induced SCD is suspected, treatment should be initiated with vitamin B12 supplementation. The British National Formulary recommended standard therapy for patients with vitamin B12 deficiency with neurologic symptoms is 1,000 mcg IM on alternating days until there is no additional improvement.14 During the patient's work-up, we recommend MRIs of the cervical, thoracic, and lumbar spine to rule out structural pathology as a cause for the patient's symptoms. Functional vitamin B12 deficiency can occur with normal serum levels of B12; therefore, a normal B12 level does not rule out this disease. In addition to specific vitamin B12 testing, plasma homocysteine and methylmalonic acid levels may be obtained. An increase in these values may indicate vitamin B12 inactivation or functional deficiency.8 Peripheral blood smears may also be obtained, and oval macrocytes, hypersegmented neutrophils, and circulating megaloblasts in the blood radiograph are typically seen with clinical vitamin B12 deficiency.14 Nerve conduction studies may provide additional supporting information as well.7 Additional laboratory studies including complete blood count should be evaluated, and vitamin B12 supplementation should be initiated if values consistent with megaloblastic anemia are seen. These laboratory values were present in our patient during her first admission to the hospital, however unrecognized at that time. In addition to spine surgeons, other specialties may be involved in these cases including neurology, internal medicine, emergency medicine, addiction medicine, and psychiatry. During their medical education, all physicians are taught the importance of folate and thiamine supplementation for patients presenting with alcohol abuse. Similarly, we hope this case report may further educate the medical community to initiate vitamin B12 supplementation in patients with this clinical picture.
To accurately diagnose and treat N2O-induced SCD of the spinal cord, a high index of suspicion is required. In addition to other medical specialties, spine surgery clinicians may be confronted with these cases and therefore should be aware of this atypical presentation of SCD. When history and physical examination are concerning for SCD, laboratory tests and advanced imaging can support the clinical diagnosis. Neurologic dysfunction may be irreversible; therefore, accurate diagnosis, medical treatment, and complete neurologic evaluation are of the utmost importance to prevent additional progression.
References 1. Koury MJ, Ponka P: New insights into erythropoiesis: The roles of folate, vitamin B12, and iron. Annu Rev Nutr 2004;24:105-131. 2. Infante M, Leoni M, Caprio M, Fabbri A: Long-term metformin therapy and vitamin B12 deficiency: An association to bear in mind. World J Diabetes 2021;12:916-931. 3. Winstock AR, Ferris JA: Nitrous oxide causes peripheral neuropathy in a dose dependent manner among recreational users. J Psychopharmacol 2020;34:229-236. 4. Garakani A, Jaffe RJ, Savla D, et al.: Neurologic, psychiatric, and other medical manifestations of nitrous oxide abuse: A systematic review of the case literature. Am J Addict 2016;25:358-369. 5. Chen W, Si Z, Bi Y, Yang B: An unusual case of subacute combined degeneration due to nitrous oxide abuse, which relapsed after bariatric surgery: A case report. Medicine (Baltimore) 2022;101:e30442. 6. Layzer RB: Myeloneuropathy after prolonged exposure to nitrous oxide. Lancet 1978;2:1227-1230. 7. Paris A, Lake L, Joseph A, et al.: Nitrous oxide-induced subacute combined degeneration of the cord: Diagnosis and treatment. Pract Neurol 2023;23:222-228. 8. Keddie S, Adams A, Kelso ARC, et al.: No laughing matter: Subacute degeneration of the spinal cord due to nitrous oxide inhalation. J Neurol 2018;265:1089-1095. 9. Beltramello A, Puppini G, Cerini R, et al.: Subacute combined degeneration of the spinal cord after nitrous oxide anaesthesia: Role of magnetic resonance imaging. J Neurol Neurosurg Psychiatry 1998;64:563-564. 10. Patel KK, Mejia Munne JC, Gunness VRN, et al. Subacute combined degeneration of the spinal cord following nitrous oxide anesthesia: A systematic review of cases [published correction appears in Clin Neurol Neurosurg. 2019 Feb;177:123-124. Abstract corrected]. Clin Neurol Neurosurg. 2018;173:163-168. 11. Oussalah A, Julien M, Levy J, et al. Global burden related to nitrous oxide exposure in medical and recreational settings: A systematic review and individual patient data meta-analysis. J Clin Med. 2019;8:551. 12. Jaiser SR, Winston GP: Copper deficiency myelopathy. J Neurol 2010;257:869-881. 13. Jung JB, Kim Y, Oh K, et al.: Subacute combined degeneration associated with vitamin E deficiency due to small bowel obstruction: A case report. Medicine (Baltimore) 2019;98:e17052. 14. Devalia V, Hamilton MS, Molloy AM, British Committee for Standards in Haematology: Guidelines for the diagnosis and treatment of cobalamin and folate disorders. Br J Haematol 2014;166:496-513.
留言 (0)