
記住我
There has been an exponential increase in the number of hip arthroscopies performed annually. The indications for hip arthroscopy have increased markedly over the past 20 years.1 A major indication for hip arthroscopy is to address symptomatic femoroacetabular impingement (FAI).2 Surgical management generally consists of arthroscopic labral débridement, labral repair, and/or contouring of the offending abnormal bony morphology of the proximal femur or acetabulum.3 Although rare, there have been a handful of cases described in which hip arthroscopy has been performed to address symptomatic paralabral cysts.4–6 There are limited case reports discussing compression of the femoral neurovascular bundle by a paralabral cyst. Kanauchi et al. described compression of the femoral nerve causing radiating nerve symptoms while Shin et al described a paralabral cyst compressing the femoral vein leading to lower extremity edema and pain.7,8 To our knowledge, there are no case reports describing compression of the femoral vein by a paralabral cyst that led to deep vein thrombosis (DVT) within the femoral vein as the first presentation of FAI.
The purpose of this report was to describe our experience treating a middle-aged woman with a paralabral cyst causing compression of the right femoral vein that led to an acute right lower extremity DVT in the setting of FAI.
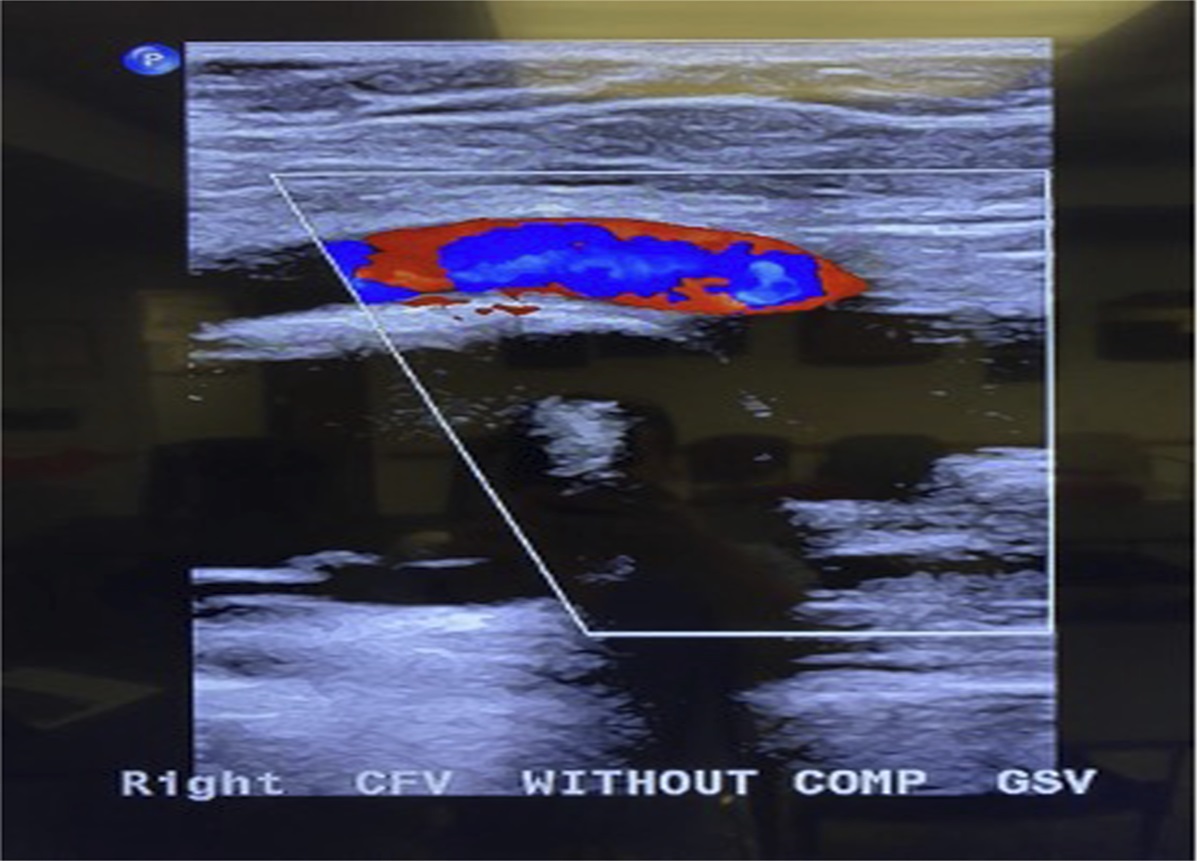
Case PresentationA 47-year-old woman was referred to our office for evaluation of a right hip paralabral cyst found on MRI. She initially presented to her primary care physician with reports of asymmetric lower extremity swelling; a palpable, painful right-sided groin mass; and mild, generalized right hip pain. She reported no history of trauma or issues with her right hip previously. A lower extremity duplex ultrasonography (US) revealed an acute occlusive DVT of the right common femoral vein, deep femoral vein, and occlusion at the saphenofemoral junction (Figures 1 and 2). She was immediately started on an oral anticoagulant, and a hematology workup was initiated to rule out causes of a seemingly unprovoked, acute DVT. The initial workup was normal. Given the presence of an associated mass in the groin and proximal location of the DVT, a pelvic MRI was ordered revealing a large anterior paralabral cyst. It appeared to originate from the joint capsule just medial to the iliopsoas tendon and clearly abutted the femoral vessels. In addition, there was evidence of a labral tear without associated subchondral cystic formation or bony edema within the acetabulum. Her plain radiographs demonstrated an anterolateral CAM-type lesion with preserved joint space (Figures 3–6).
 Figure 1:
Figure 1: Diagnostic US image of the right groin demonstrating an occlusive DVT in the common femoral vein adjacent to a large hypoechoic mass. DVT = deep vein thrombosis
 Figure 2:
Figure 2: Labeled cross-sectional US image of the right groin demonstrating a large, hypoechoic mass causing mass effect on the common femoral vein near its communication with the greater saphenous vein.
 Figure 3:
Figure 3: Preoperative AP radiograph of the pelvis.
 Figure 4:
Figure 4: Preoperative lateral radiograph of the femur revealing a moderate-sized CAM lesion of the anterolateral femoral head/neck junction.
 Figure 5:
Figure 5: Preoperative false profile radiograph demonstrating preserved joint space as well as normal head/neck offset and anterior femoral head coverage.
 Figure 6:
Figure 6: Axial T2-weighted MRI of the right hip demonstrating a labral tear with associated anterior paralabral cyst adjacent to and compressing the femoral neurovascular bundle.
Treatment options were discussed in detail and included cyst aspiration versus hip arthroscopy. Image-guided aspiration of the cyst was thought to be the lowest risk option, but would be associated with a high risk of recurrence because of her labral pathology. Regarding arthroscopy, she would be required to stop her anticoagulation 48 hours before surgery, which could increase the risk of DVT propagation and possible embolization, particularly with the use of intraoperative traction. Vascular surgery recommended inferior vena cava (IVC) filter placement before arthroscopy. After multiple discussions and a shared decision-making process, it was decided to proceed with IVC filter placement, followed by hip arthroscopy with cyst decompression, labral repair, and femoral and acetabular osteoplasty.
Surgical TechniqueSurgery was performed in a hospital-based surgery center under general anesthesia. A designated vascular surgeon was notified of the timing of the case and was available to assist in the event of inadvertent arterial or venous injury during decompression given the location of the cyst.
The patient was positioned on a traction table in the supine position. A right hip arthroscopy was performed using a standard anterolateral viewing portal and mid-distal anterior portal, made under direct visualization. After performing an interportal capsulotomy, we inspected the hip joint. Diagnostic arthroscopy revealed mild chondral delamination beginning posteriorly on the acetabulum and extending anteriorly to the weight-bearing surface. The cartilage of the femoral head appeared to be intact. Evaluation of the labrum revealed a full-thickness 270° tear corroborating MRI results (Figures 7 and 8).
 Figure 7:
Figure 7: Arthroscopic image of the right femoral head and acetabulum.
 Figure 8:
Figure 8: Arthroscopic image of the labral tear.
First, an acetabuloplasty using a burr followed by labral repair with six knotless all-suture anchors was performed (Figure 9). With the labrum repaired, the cyst entrance was now closed off. Attention was then turned to the anterior capsule, which was dissected bluntly to identify the iliopsoas tendon. A Z-lengthening of the iliopsoas was performed using radiofrequency ablation. The cyst wall was encountered with additional blunt dissection. The cyst wall was carefully opened, drained, and débrided with great care taken not to extend too medially to encounter the neurovascular bundle (Figure 10). Most of the cyst was débrided, but the entirety could not be removed without causing unnecessary risk to the neurovascular bundle. In addition, the cyst was very difficult to access using the available arthroscopic instruments given its location and the patient's BMI of 35. Multiple shavers and ablators were bent or broken in attempts to débride the cyst in its entirety. For these reasons, we did not continue to attempt a full decompression because we did not want to risk injuring the neurovascular bundle. After our best attempt at cyst decompression, we performed osteoplasty of the anterolateral femoral neck. Finally, capsular closure completed the procedure.
 Figure 9:
Figure 9: Arthroscopic image of the repaired labrum.
 Figure 10:
Figure 10: Arthroscopic image of the paralabral cyst entrance adjacent to the iliopsoas tendon.
Postoperative CoursePostoperatively, the patient was made partial weight-bearing and instructed to avoid active and resisted hip flexion for 8 weeks. She restarted an oral anticoagulant on postoperative day one. Physical therapy was started immediately and consisted of light, low-resistance cycling, stretching, and passive range of motion. She was given a 1-month course of Indocin and Naprosyn 500 mg BID to prevent heterotopic ossification. At 2 weeks, she was doing well regarding pain and mobility. A repeat pelvic MRI was planned for the 3 months postoperatively to look for cyst resolution. Discussion was had that IVC filter removal should be delayed until confirmation of cyst eradication. At 6 weeks, she demonstrated 100° of hip flexion and was progressing well with therapy.
At 3 months, the patient's MRI unfortunately revealed persistence of the paralabral cyst in the same location, with similar appearance to her preoperative MRI (Figure 11). The labral repair, fortunately, did appear intact. Given these findings, we discussed image-guided decompression with interventional radiology (IR) now that the labrum was repaired. Despite persistence of the cyst, vascular surgery thought it was safe to discontinue anticoagulation and remove the IVC filter. Promptly thereafter, IR performed an US-guided aspiration of the cyst. One month later, follow-up US revealed complete cyst eradication. A third MRI 2 months after aspiration confirmed complete cyst resolution (Figure 12).
 Figure 11:
Figure 11: Axial T2-weighted MRI 3 months postoperatively demonstrating cyst persistence.
 Figure 12:
Figure 12: Axial T2-weighted MRI after US-guided cyst aspiration demonstrating resolution of the cyst and an intact labrum.
The patient is now over 2 years out from surgery and doing well without pain or functional concern.
DiscussionLimited reports of paralabral cysts causing compression of nearby neurovascular structures exist.5,7,8 To our knowledge, none have reported cysts as a cause of acute DVT. As a result, there are no clear guidelines on how to treat this uncommon condition. Although this patient's presentation is anomalous, this report serves as evidence to include FAI and resultant labral pathology with cyst formation as an item on the differential diagnosis for a proximal, seemingly idiopathic DVT in the lower extremity. We hope that our experience can help guide future treatment plans and help develop more regimented treatment algorithms.
Hip arthroscopy is a difficult procedure at baseline. The added challenge of visualizing and decompressing a cyst adjacent to the femoral neurovascular bundle creates an exceedingly difficult task. Many factors should be considered, including patient BMI. In this case, we bent and even broke several instruments attempting to decompress the cyst. With postoperative MRI showing persistence of the cyst in the same location, it is evident that we did not fully decompress the cyst. Much less likely possibilities include blood infiltration after the procedure or that it simply recurred.
There are several learning points that can help guide future treatment of this uncommon entity. The first and most important involves the sequence of diagnostic and therapeutic interventions. This patient may have been able to avoid inadequate cyst débridement and ultimate recurrence as well as experience a quicker overall time to resolution with a more coordinated sequence of events. Clearly, arthroscopic decompression was not sufficient to address the paralabral cyst; however, we believe that labral repair to seal the cyst entrance is paramount to prevent recurrence.
In hindsight, arthroscopic labral repair and ultrasonography-guided drainage of the cyst could have been strategically performed in concert with the patient under anesthesia in the OR or very soon following hip arthroscopy. In future cases, we plan to have IR perform perioperative cyst decompression either immediately before or immediately after hip arthroscopy while the patient is still under anesthesia. This would have possibly eliminated the need for an IVC filter and likely decreased the overall duration of systemic anticoagulation for our patient.
ConclusionEven in the most experienced hands, unusual cases such as this present diagnostic and logistical conundrums. Hip arthroscopy with labral repair followed by US-guided aspiration either intraoperatively or in the early postoperative period likely would have resulted in quicker resolution of symptoms for this patient. Future cases of paralabral cysts causing mass effect should be treated with hip arthroscopy and image-guided aspiration in a concerted effort.
References 1. Palmer AJ, Malak TT, Broomfield J, et al.: Past and projected temporal trends in arthroscopic hip surgery in England between 2002 and 2013. BMJ Open Sport Exerc Med 2016;2:e000082. 2. Lee KH, Park YS, Lim SJ: Arthroscopic treatment of symptomatic paralabral cysts in the hip. Orthopedics 2013;36:e373-e376. 3. Nwachukwu B, Rasio J, Sullivan S, Okoroha K, Mather RC, Nho SJ: Surgical treatment of labral tears: Debridement, repair, and reconstruction. Sports Med Arthrosc Rev 2021;29:e1-e8. 4. Bystrom S, Adalberth G, Milbrink J: Giant synovial cyst of the hip: An unusual presentation with compression of the femoral vessels. Can J Surg 1995;38:368-370. 5. Kullar RS, Kapron AL, Ihnat D, Aoki SK, Maak TG: Acetabular paralabral cyst: An unusual cause of femoral vein compression. Arthrosc Tech 2015;4:e35-e40. 6. Magee T, Hinson G: Association of paralabral cysts with acetabular disorders. AJR Am J Roentgenol 2000;174:1381-1384. 7. Kanauchi T, Suganuma J, Mochizuki R, Uchikawa S: Arthroscopic treatment of femoral nerve paresthesia caused by an acetabular paralabral cyst. Orthopedics 2014;37:e496-e499. 8. Shin KY, Park SJ, Lee WS: Paralabral cyst of the hip compressing common femoral vein treated with sono-guided cyst aspiration followed by arthroscopic labral debridement: A case report. Hip Pelvis 2017;29:194-198.
留言 (0)