We examined the relationships between teacher and parent reports of primary school children’s mental health and neighbourhood area deprivation over time. We found an association between living in a socioeconomically deprived area and SDQ total difficulties scores from both informants across the three time-points. We found no such association for probable disorder, which we explore further below. The relationship between mental health and SEND is complex [10]; neurodevelopmental conditions in themselves can require support for children to cope with school, while other types of SEND can precipitate mental health conditions and both SEND and mental health conditions are commoner among those of lower economic status. We, therefore, included a sensitivity analysis to explore the effect of SEND, which attenuated the association with all outcomes although the relationship of IMD and mental health remained related (p < 0.001) according to parent report. Our main analysis excluded SEND as the study we aimed to replicate did not include it, and because of the complexity of variable that for different children may be a confounder, a mediator or a risk factor.
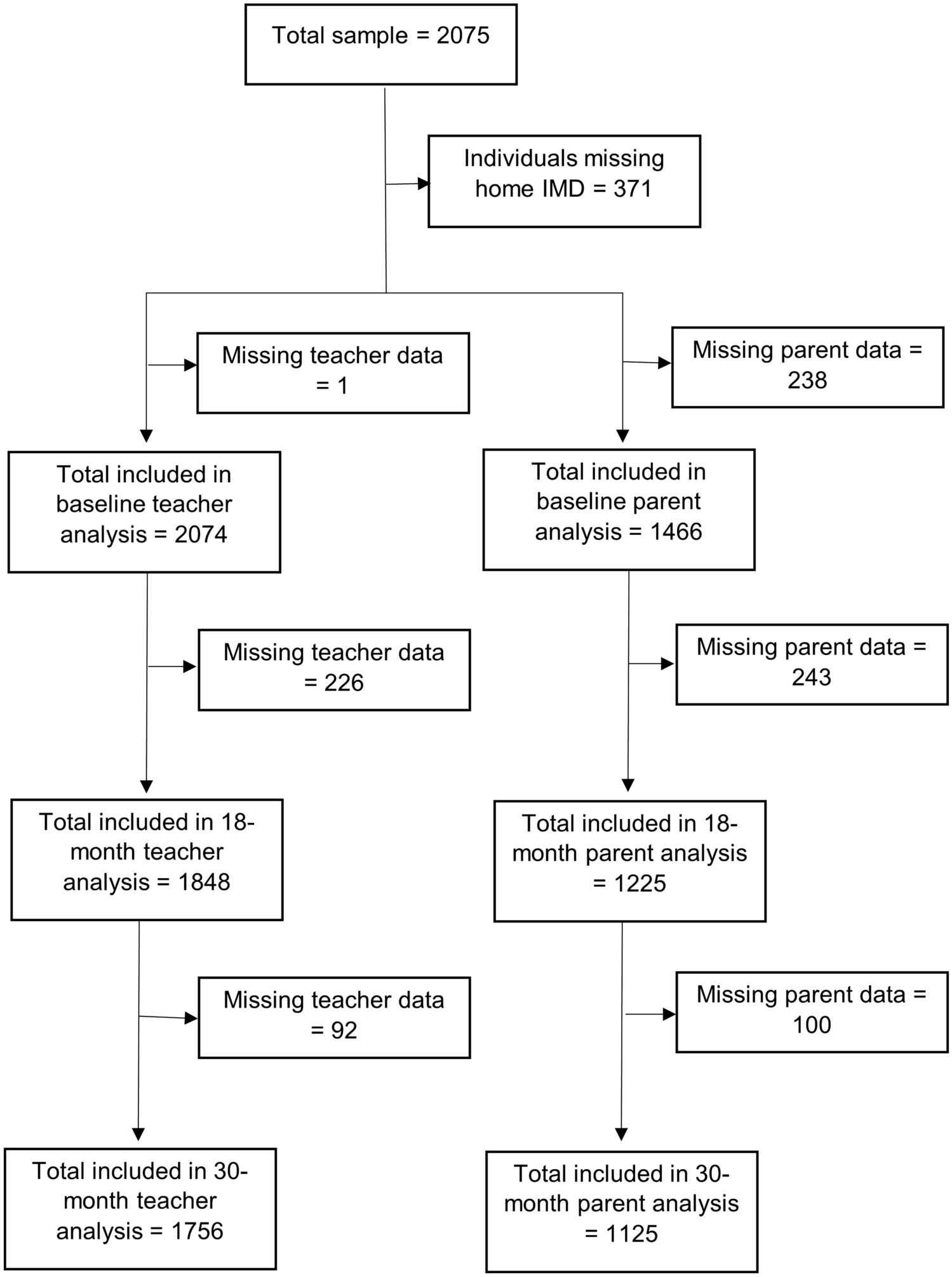
We failed to replicate the widening of the disparity in mental health by socioeconomic deprivation with age that was reported by Marryat et al. [7]. Time related findings may result from an age effect (mental health deteriorates with age); a cohort effect (related to the particular population of children starting school) or a period effect (relating to children more widely in that context and that date, usually due to particular socio-political events). The latter seems unlikely as data were collected in similar time periods, and although the studies were in different countries with some differences in education and health policy, they are both part of the UK. There are also important methodological differences between their study and ours. This Scottish study was both larger (3166 participants) and all the children shared the same year group and age; the authors dichotomised the SDQ scores; and did not formally test for an interaction with time, although the graphical illustration reported is compelling. In contrast, STARS recruited 2075 children divided across five school year groups, so had less statistical power to detect differences in the relationships across a wider range of ages.
Dimensional measures provide greater statistical power to detect an association than binary variables, which may explain our failure to detect of an association for probable disorder. Our findings might also result from an affect that does not differentially influence those with poorest mental health but operates across the distribution of scores. The SDQ diagnostic algorithm most accurately predicts disorder when combining parents’ and teachers’ reports for this age group, as we did, compared to teacher or parent only report [18,19,20]. Multi-informant assessment is more accurate than single informant as is the use of impairment as well as symptoms, hence our inclusion of this measure [24]. However, the algorithm’s performance as a diagnostic test is moderate [24], and although better than a cutpoint in symptoms alone, misclassification may also explain our failure to detect an association with caseness. We used the conventional classification (probable versus, unlikely / possible) as it is likely that shifting the cutpoint to probable / possible versus unlikely would serve to increase misclassification and to move the measure further away from clinical diagnoses.
The interaction of probable disorder with time may be a chance finding, particularly lack a similar interaction with parent and teacher SDQ total difficulties scores, for which there was a clear main effect. There is no theoretical reason why those living in deprived areas should be at higher probability of psychiatric disorder at baseline and 18 months but not 30 months.
Interestingly, our findings suggest that a stronger association between parent-reported mental health and IMD. Teacher and parental agreement on mental health measures is surprisingly low [25], although Marryat and colleagues relied on teacher report. For some children, there will be a true difference in how children function at home and at school, as many children, particularly those with anxiety or neurodevelopmental disorders, contain or mask their difficulties in school and then decompensate at home. Parents with a lower socioeconomic status are more likely to have poorer mental health themselves, and their mental state may influence how they score their children on the SDQ [26]. Evidence supports such a reporting bias but direct observation also suggests their children also have more difficulties, and there is no reason for parental reporting bias among respondents to only manifest at baseline and 18 months [27]. The percentage of individuals meeting multi-informant standardized diagnostic assessment for an impairing DSM IVR diagnosis whose algorithm-derived variable indicated probable disorder was 50%, compared to 11% for possible and 2% for unlikely [20]. There is a risk that the relationship between deprivation and diagnosable psychiatric disorder might have been obscured by misclassification, although the use of impairment and multiple informants improves on the use of a simple cutpoint as applied by Marryat and colleagues. While our parent reports reflect national survey data, our teacher reports indicated greater psychopathology among the STARS participants, which probably reflects methodological differences. The national survey recruited parents and requested access to teachers, but not all families accepted and not all teachers responded. Teacher information in the national survey was less likely to be available for children reaching diagnostic criteria for mental health conditions and of lower socioeconomic status.
The children participating in our study experienced a very different environment than the Scottish study, albeit at a similar period (2012–2015 Marryat vs. 2012–2017 STARS). STARS recruited schools from mainly rural and semi-rural areas in South-West England compared to a large Scottish city. Although both samples were living in countries within the UK, England and Scotland differ substantially in the provision of education and social care. Notably, the regions from which the data were collected show similar levels of wealth inequality as measured by the Gini coefficient (59% South-West England and 62% Scotland, respectively) [28]. Some evidence suggests that access to rural areas may be beneficial to mental health, which perhaps might mitigate the impact of deprivation [29,30,31,32]. Further research could explore whether this is the case among young children.
Others argue strongly about the deleterious impact of the widening gap between the most and least privileged of British society [33] and given that our findings add to the robust literature that the mental health of children living in poverty seems generally poorer, there is an urgent necessity to support vulnerable children and families, as suggested by Fazel [34]. The Covid-19 pandemic has amplified the significant deterioration in young people’s mental health seen in the first 2 decades of this century [23, 35], with repeated reports that children living in deprived areas or lower socioeconomic status families were more likely to experience poor mental health than their peers who were not facing such challenges [36,37,38]. The school closures and disruption to education resulting from COVID-19 is predicted to increase the gap in education outcomes between children from poorer and affluent families [11]. Children with pre-existing mental health conditions and SEND were particularly likely to experience poor mental health during the pandemic [37]. Furthermore, there is increasing evidence of the syndemic impact of COVID-19 and resulting restrictions, with vulnerable groups facing multiple challenges that did not affect other sectors of society [39,40,41]. For example, in a study that compared mental health trajectories during 2020, adults from ethnic minorities, people living in more socioeconomically deprived circumstances and parents with young children, were more likely than their White, more affluent and childless peers to experience deteriorating or consistently poor mental health [42]. We should be particularly concerned that parents of young children emerged as a novel high-risk group [42], given the strong bidirectional relationship of parental and child mental health [43]. This association unique to parent–child connections may offer explanation towards the more pronounced correlation between deprivation and parent-reported SDQ total difficulties score as opposed to those scores reported by teachers. Parents raising children in areas experiencing more deprivation may not only struggle more with mental health difficulties themselves but also be more acutely aware of these difficulties in their children [42, 43].
We need a concerted cross-sector policy to support children and families, which should comprise universal, targeted and indicated measures with a focus that is broader than just mental health. We found that adjusting for SEND attenuated the relationship between deprivation and mental health according to all three outcomes, although the association remained intact (p < 0.001) according to parental report. It is essential that children who struggle at school are adequately supported. Prevention should support parenting, provide high-quality affordable childcare and ensure children are adequately fed and housed. Either universal or targeted screening, if linked to effective intervention, might reduce the developmental price of untreated mental health difficulties. Children might also be more likely to respond to intervention if they access support before their difficulties become entrenched [44]. A study of schools in socially deprived areas found that 82% of parents agreed that regular mental health screening in primary schools would be beneficial for students [45], although subsequent access to support needs careful consideration. Mental health services for children are already struggling to deal with referrals, with evidence that many with clinically impairing difficulties struggle to access care [37, 46, 47]. Therefore, we need to ensure that scarce specialist resources are used cost-effectively and to upskill and support all professionals who work with children and young people to provide effective help for milder and transient problems and to identify those who need more active intervention. The aspiration to significantly expand access to high-quality community mental health services to meet the needs of 35% of young people in need by 2021 should aim for complete coverage and risks being swallowed by increasing demand [48, 49]. A focus on economically deprived areas might help target resources where they are most needed and may reduce both individual burden on sufferers and systematic burden on health, social care and education services [50].
There are several strengths to our partial replication, which include the use of a moderately large sample, followed prospectively and the use of a widely used validated outcome measure. We extend Marryat’s work by the inclusion of parents as well as teacher SDQs and the algorithm-generated “probable disorder”. Inevitably, there are constraints with missing parental reports (and, therefore, demographic information and home—IMD), which increased over time. It seems likely that a high proportion of parents who chose not to respond or dropped out of the study were from lower socioeconomic backgrounds [51]. The schools recruited were representative of schools in the South West of England, but we excluded from the trial schools deemed to be unsatisfactory on inspection, which are likely to serve particularly deprived catchment areas [15]. Similarly, the South West of England is an area of low ethnic diversity, so our findings cannot be generalised to more ethnically mixed neighbourhoods.
We chose IMD as our measure of deprivation given our aim to replicate Marryat’s work, which used the Glasgow IMD [7]. IMD was also preferred as it considers a number of markers in its calculation, making it an effective marker of area-level deprivation [16, 17]. IMD has been praised for its use as a comprehensive indicator of area-level deprivation, used by governmental bodies and directing attention to areas in need. However, challenges include those ascribed to each of the 37 included measures, and the IMD assumes that of each of these measures are experienced similarly by the all individuals in each area [52]. Our work could not explore indictors of individual level socioeconomic status such as eligibility for free school meals and the highest level of parental education, which we did use to impute data, because these characteristics are collinear with our outcome measure.
More generally, residual confounding may explain the finding of an interaction between IMD, probable disorder and timepoint. Further research should seek to replicate our work exploring the mental health gap between children by neighbourhood deprivation in larger datasets and over a wider age-range.


留言 (0)