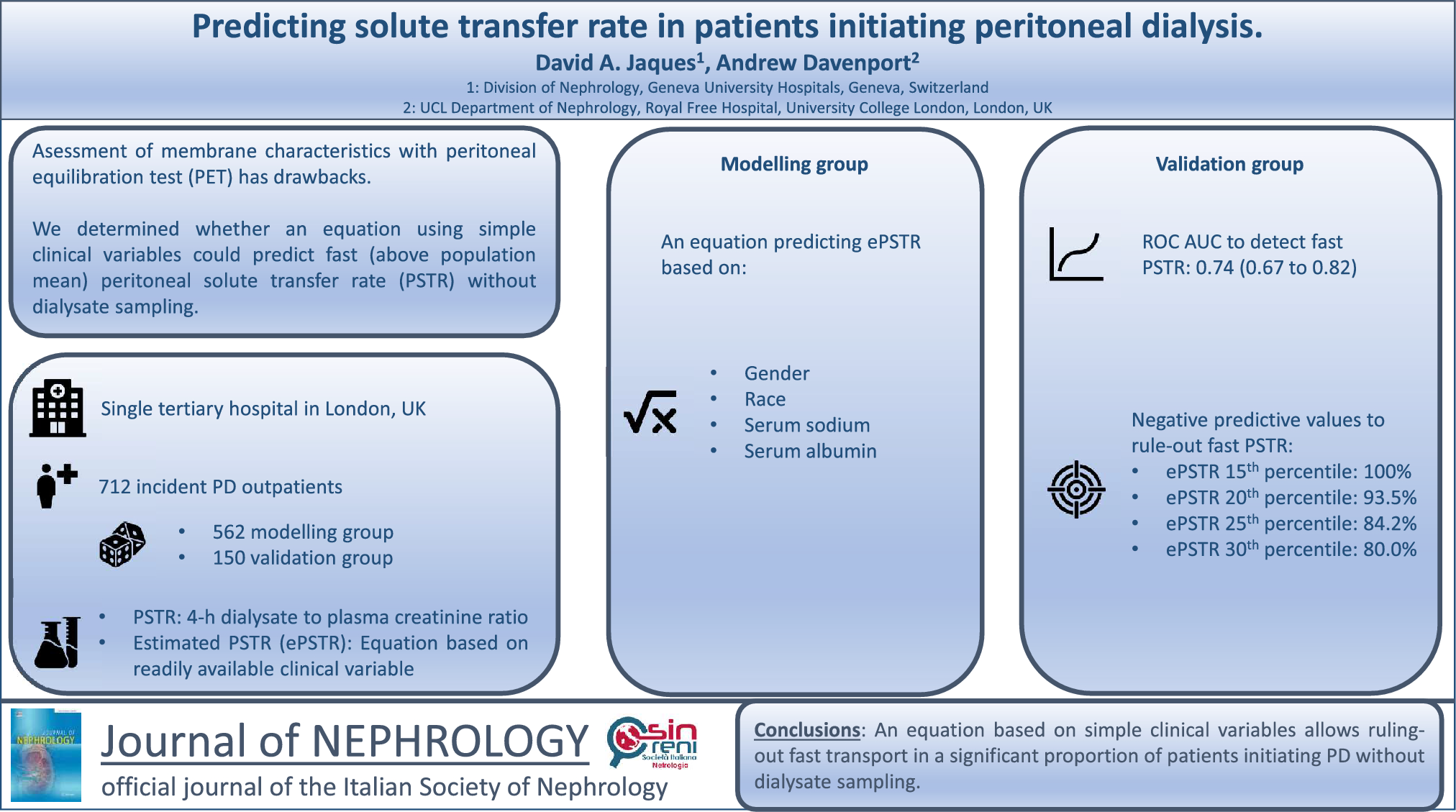
In this study, we described predictors of peritoneal solute transfer rate in incident patients recently starting PD, and developed an equation using readily available clinical parameters to predict transport status without relying on dialysate sampling. Although offering overall moderate performance that can not replace formal peritoneal equilibration test assessment in every clinical setting, this equation allows screening of incident patients starting PD to reliably rule out fast transporters.
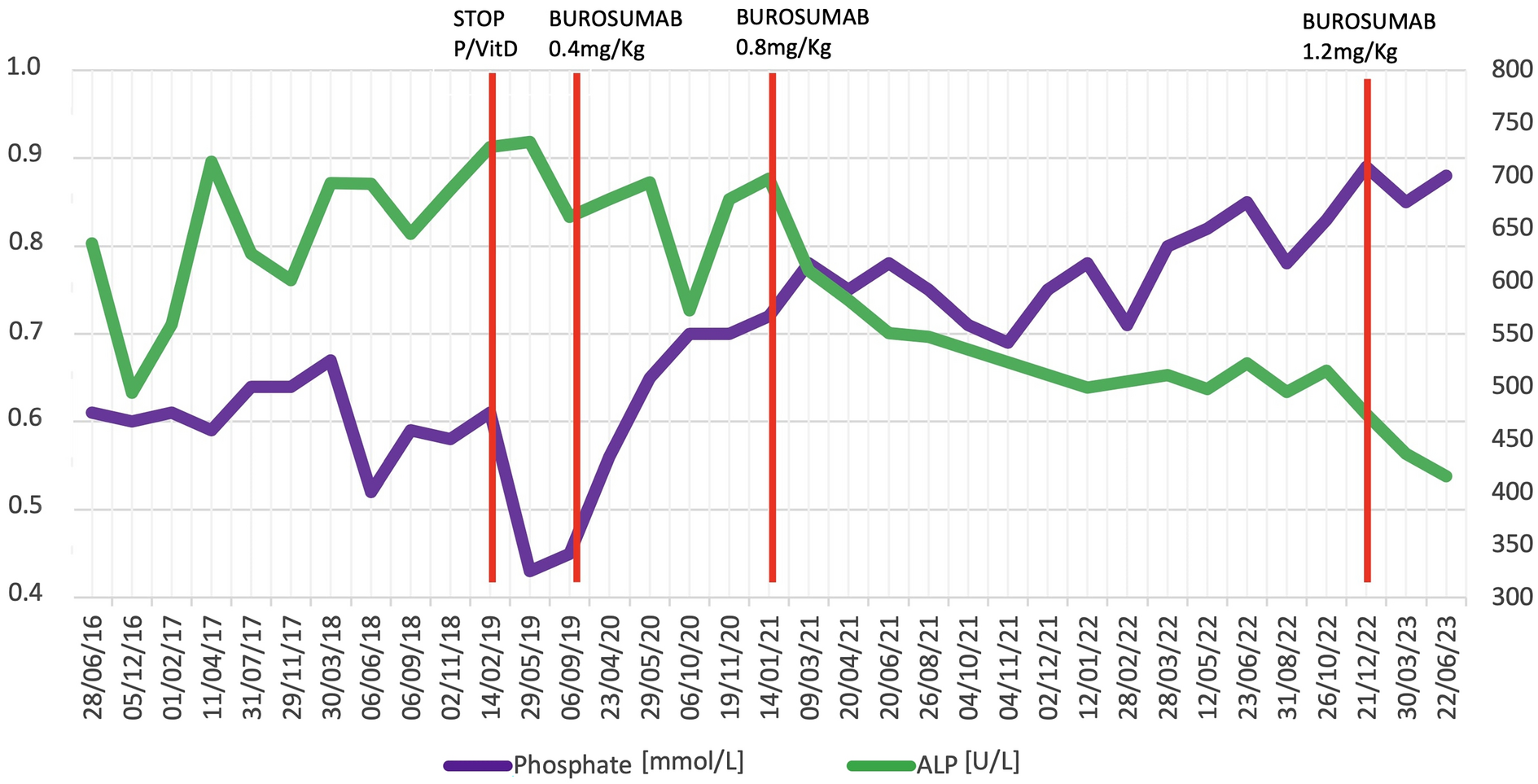
It has long been observed that inter-individual variability in peritoneal solute transfer rate is high at dialysis initiation. In the present study, we report a mean peritoneal solute transfer rate value of 0.73 ± 0.13. In prior cohorts including patients from Oceania, the US and the UK, mean peritoneal solute transfer rate was slightly lower, while an Italian group reported a value strictly identical to ours [9, 12,13,14]. In comparing those numbers, one must bear in mind that variability could arise not only from inherent clinical differences between various studied populations but also from the lack of strict analytical standardization of peritoneal equilibration test assessment [3, 12, 13]. Predictors of peritoneal solute transfer rate at dialysis initiation are still poorly understood with very heterogeneous results among main studies [9, 12, 13, 15]. In our cohort, gender, serum albumin and serum sodium were the three factors with the highest effect size on peritoneal solute transfer rate at dialysis initiation. Specifically, fast transport was associated with male gender as well as lower albumin and sodium serum levels. The gender effect on peritoneal solute transfer rate is well documented and is generally thought to be explained by the relative larger size of men as compared to women as the 3-pore model predicts that transport rate increases when a larger membrane surface area is in contact with the dialysate [12, 13, 15]. In keeping with this hypothesis, the gender effect tended to disappear when accounting for body surface area in prior reports [9, 13]. Conversely however, we observed that male gender remained a strong determinant of fast transport while accounting for body surface area as well as other confounders, potentially suggesting an association with the functional vascular peritoneal area in addition to the anatomic membrane area. Lower serum albumin was previously associated with higher transport rate and has been thought to mediate the relationship between peritoneal solute transfer rate and clinical outcomes, as a global marker of frailty [9, 13]. Peritoneal protein loss could explain the low serum albumin in fast transporters. However, an association between peritoneal solute transfer rate and albumin has been noted prior to dialysis initiation [16]. Alternatively, underlying chronic inflammation could also explain both low albumin and fast transport rate,but, then again, most studies failed to identify a relationship between peritoneal solute transfer rate and inflammatory parameters [17, 18]. Our findings support a direct link between transport status and albumin levels as this relationship remained highly significant despite adjusting for comorbidities and C-reactive protein. Finally, while not previously described in prior publications, we also found that fast transporters had lower serum sodium. An increase in intra-vascular free water is the most likely explanation to this phenomenon as it was previously shown that fast transport allowed relatively more sodium to be removed as compared to water in those patients [19]. This is also corroborated by a positive association between extracellular water/total body water and peritoneal solute transfer rate in our cohort. Conversely, slow peritoneal transport could magnify sodium sieving and hamper sodium removal when short dwells are prescribed. Lastly, the influence of PD mode (CAPD vs APD) must be remembered as dialytic sodium removal was shown to be less efficient relative to water removal with APD as compared to CAPD [19]. This would support the hypothesis that shorter dwell used in APD favors sodium sieving and water removal through aquaporins that cannot be compensated by later convective transfer of sodium. The present work was however not designed to confirm those physiological hypotheses and the interested reader might refer to a previous publication [19].
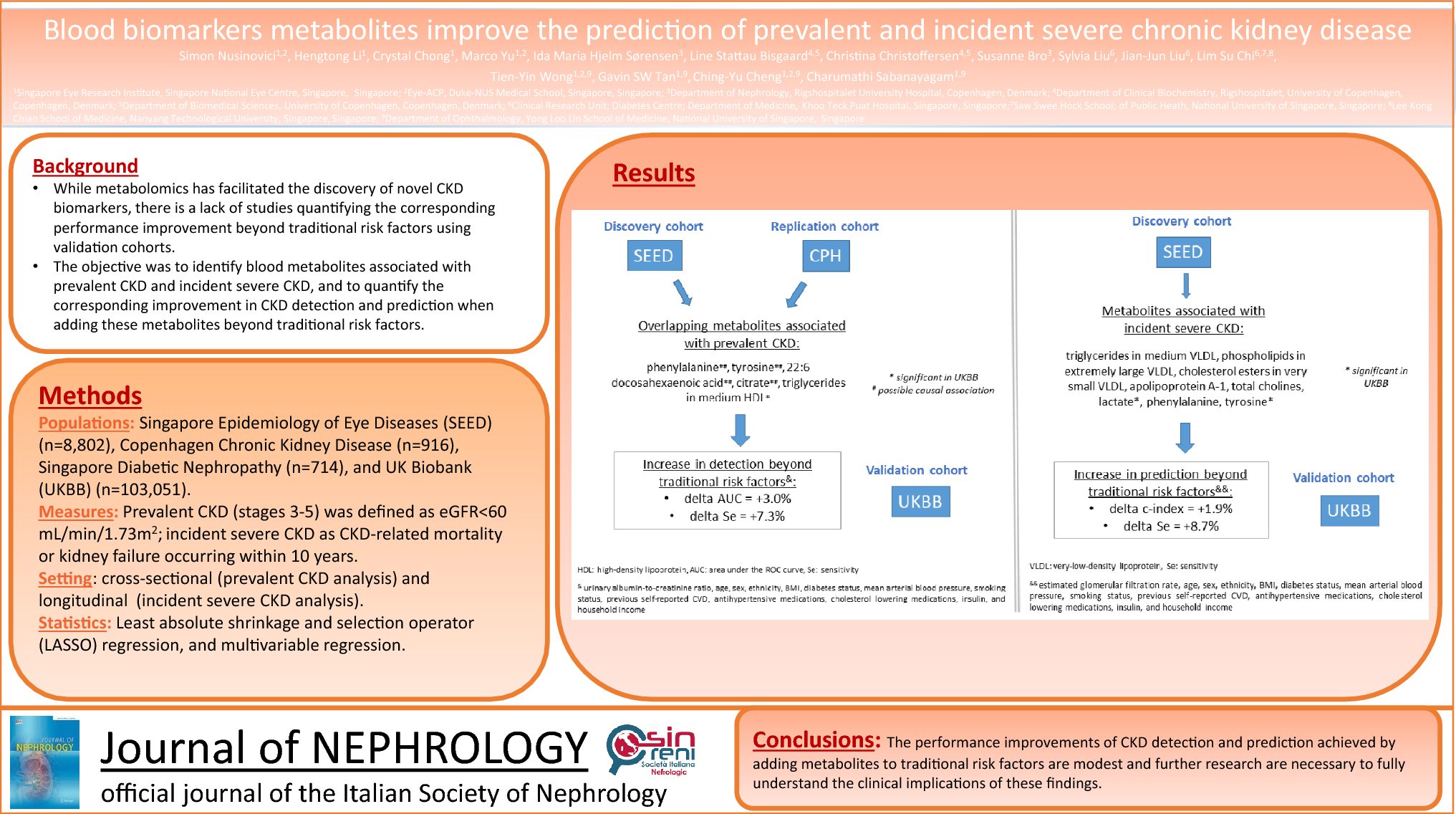
The main finding of our study is the potential clinical application of an equation based on readily available clinical variables to predict transport status in incident PD patients without relying on dialysate sampling. Our equation is obviously not intended to universally replace formal peritoneal equilibration test assessment as it allows estimation of a single metric (peritoneal solute transfer rate) with moderate accuracy only. Our model could thus only explain 18.4% of peritoneal solute transfer rate variance observed in the validation group. We believe however that it could have clinically meaningful applications as detection of fast peritoneal solute transfer rate is important to guide PD prescription in daily practice [3]. Using our equation, an estimated peritoneal solute transfer rate cut-off above the 15th (> 0.66), 20th (> 0.68), 25th (> 0.69) and 30th (> 0.70) percentiles could rule out fast peritoneal solute transfer rate (> 0.73) with negative predictive values of 100%, 93.5%, 84.2% and 80.0%, respectively. That performance allows exclusion of fast peritoneal solute transfer rate at dialysis initiation in a significant proportion of patients with high clinical certainty. Such information could potentially be used in incident patients to guide initial PD prescription prior to peritoneal equilibration test assessment as well as later during follow-up to ensure adequacy of dialytic therapy.
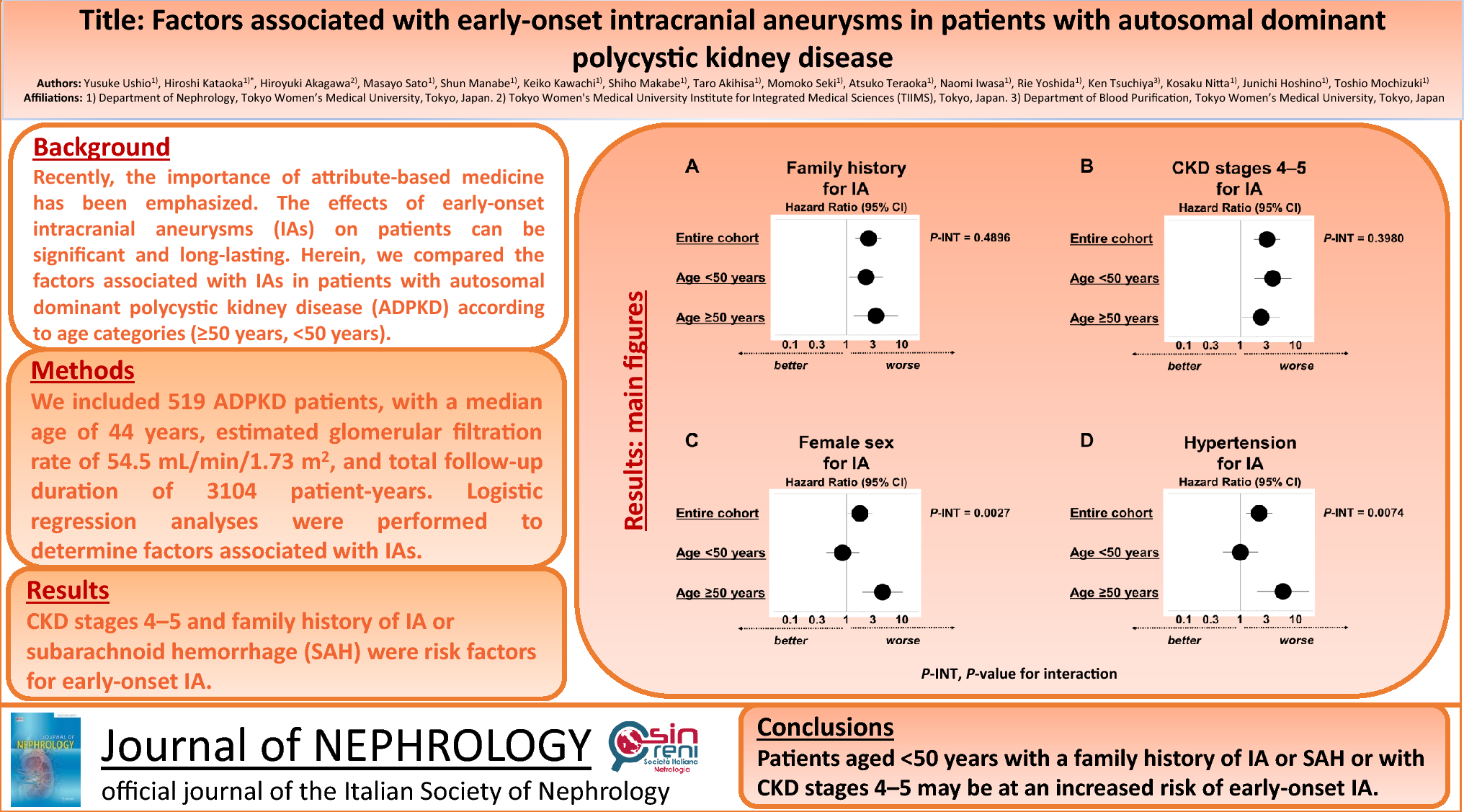
Peritoneal solute transfer rate values show significant regional discrepancies owing to differences in populations as well as procedural and laboratory standardization [3, 9, 12,13,14]. However, peritoneal solute transfer rate is normally distributed with a very reproducible standard deviation across various populations [3]. It is also reproducible within a given individual with a coefficient of variation < 10% within a month of testing [3]. Consequently, we chose to develop a predictive model based on relative peritoneal solute transfer rate values, based on mean and percentiles thus potentially allowing direct application to other populations with different absolute peritoneal solute transfer rate values. It is also worth noting that our model only uses four readily available variables (gender, race, serum albumin and serum sodium) to achieve discrimination. As such, it could be potentially implemented in many clinical settings, even those with particularly low resources. Using our equation, negative predictive values (rule out) were notably higher than positive predictive values (rule in) to detect fast peritoneal solute transfer rate. This is however expected by design as we deliberately chose cut-offs that would allow exclusion of fast peritoneal solute transfer rate, a result that would have the most impact regarding clinical decisions at dialysis initiation. While prior publications described various equations aiming at estimating residual kidney function without relying on 24-h urine collection, we could not find comparable studies focusing on peritoneal solute transfer rate estimation [20,21,22]. Our results could thus not be compared with those of other groups and should rather constitute a springboard to future research.
Readers should bear in mind several limitations when interpreting our findings. First, our study is cross-sectional in nature and longitudinal follow-up was not available in our cohort. Consequently, our findings would apply to incident patients only and performance of our equation to detect later changes in peritoneal solute transfer rate during follow-up could not be assessed. This aspect should be addressed before considering application in a real-life setting. Second, similar to most publications focusing on non-invasive predictive equations, we used an internal validation procedure that should be externally validated before considering pragmatic application [20,21,22]. Overfitting of our model was however prevented by randomly splitting our cohort into two distinct groups of satisfactory sizes. Moreover, in agreement with the latest guidelines, we used relative peritoneal solute transfer rate measurements (mean and percentiles) and not absolute values. We could thus rely on the reproducibility of peritoneal solute transfer rate distribution across populations without using center-specific peritoneal solute transfer rate absolute values. Finally, our equation includes self-reported race that has been criticized as a sociopolitical construct mediating the effect of structural racism in estimating glomerular filtration rate [23]. In the present setting however, we believe that this should be tempered as classifying solute transfer rate in PD patients is obviously not as sociologically delicate as the estimation of kidney function.


留言 (0)