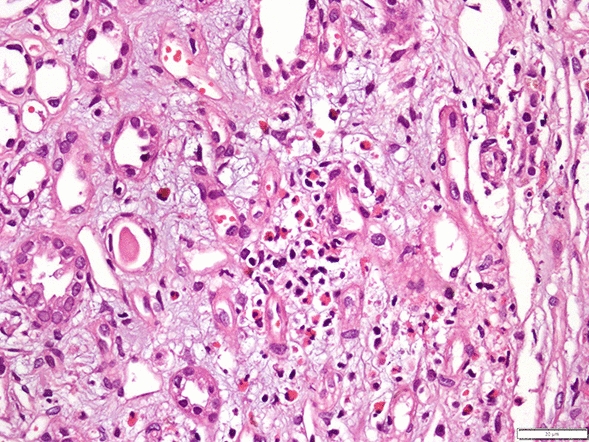
Here we report the co-existence of rhabdomyolysis and acute interstitial nephritis. It was not possible to identify the exact cause of acute interstitial nephritis in this patient. Rhabdomyolysis most likely developed as a result of the patient’s long time on the run. Considering the wounds that were observed all over his body, he may have also suffered trauma. While rhabdomyolysis may cause intratubular casts, induce reactive oxygen species and tubular necrosis [1], acute interstitial nephritis due solely to rhabdomyolysis is not likely [2]. As the patient reported no use of drugs nor did he have any opportunity to get them, the agent causing acute interstitial nephritis might have been a plant, fruit or an insect bite. Another possibility is that a common insult, such as an infectious agent or a snake toxin, caused both rhabdomyolysis and acute interstitial nephritis [3, 4]. However, the clinical history was silent in this regard.
While we can not find the exact reason for concomitant rhabdomyolysis and acute interstitial nephritis in this patient, it is conceivable that the ultimate cause has to be ascribed to his refugee status. Although he felt that he had to run away and hide in the forest to save his life, this exposed him to hazardous factors. His temporary protection status in Turkey gave him the chance to receive all the necessary treatments free of charge. The patient stated that he considered himself lucky to have his kidney health back.
Turkey currently hosts the largest refugee population in the world, with an estimated 4 million individuals [5]. Although the basic healthcare needs of the refugee population are similar to those of residents, they are more vulnerable to acute diseases, mostly because they are often on the brink of survival due to poor living conditions.
Refugees in Turkey, the majority of whom come from Syria, try to cross the western borders of the country into Greece and Bulgaria to reach Europe, in the quest for a better life. This is why many try to flee across the borders or cross the Aegean Sea [6]. Unfortunately, they face additional, potentially deadly risks during their journey. The unpredictability of their situation is challenging not only for them but also for the authorities and medical staff who take care of them.
To our knowledge, this is one of the very few reports of a rather unusual presentation of AKI in a refugee patient. The underlying pathology of AKI in this patient, which involved both rhabdomyolysis and acute interstitial nephritis, may suggest considering the entity of “refugee nephropathy”, a hypothesis that needs validation, gathering further similar cases. Rhabdomyolysis may be frequent in refugees and migrants because extreme physical activity, trauma, crush syndrome, toxins and infections can result in muscular injuries, while infectious agents and toxins may cause acute interstitial nephritis. Our experience with this patient shows that both can be seen concomitantly. There are some previous examples of unusual presentation of diseases in underserved populations [7, 8].
Beyond acute diseases, caring for chronic kidney disease (CKD) in refugees is also challenging [9]. Many do not have timely access to proper care. This may increase the burden of emergent conditions for refugees with chronic kidney disease.
In conclusion, as they face poor living conditions, refugees are vulnerable to health risks. Because of their unusual exposures, they may have different disease patterns and may be simultaneously exposed to different causative factors. Nephrologists should bear in mind that different etiologic factors and disease patterns may coexist in refugee patients and they should modify their diagnostic algorithm accordingly.


留言 (0)