
記住我


A total of 15 patients were enrolled in part E of the KEYNOTE-011 study between March 10, 2017, and February 28, 2020 (data cutoff): 6 patients in cohort 1 (pembrolizumab plus cisplatin and etoposide), 6 patients in cohort 2 (pembrolizumab plus carboplatin and etoposide), and 3 patients in cohort 3 (pembrolizumab plus cisplatin, etoposide, and prophylactic pegfilgrastim). Database lock was June 11, 2020.
Patient characteristics are summarized in Table 1. Median age was 63.5 years in cohort 1, 65.0 years in cohort 2, and 57.0 years in cohort 3. Overall, median age was 64 years, and approximately half of patients included in the study were men. Three patients in cohort 1, 1 patient in cohort 2, and 1 patient in cohort 3 had brain metastases at baseline.
Table 1 Patient demographics and baseline clinical characteristicsMedian time from treatment allocation to data cutoff (February 28, 2020) was 16.1 months (range, 4.1‒31.4 months) for cohort 1, 17.7 months (range, 6.4‒32.4 months) for cohort 2, and 22.1 months (range, 8.9‒25.6 months) for cohort 3. Across all 3 cohorts, median time from treatment allocation to data cut off was 22.1 months (range, 4.1‒32.4 months). All patients discontinued study treatment due to PD (n = 12), AEs (n = 2), or physician decision (n = 1; Fig. 1). Median treatment exposure was 2.8 months (range, 0.1‒13.4 months) in cohort 1, 4.5 months (range, 2.2‒7.7 months) in cohort 2, and 3.5 months (range, 3.5‒4.9 months) in cohort 3. Median number of pembrolizumab administrations was 5 (range, 1‒19) in cohort 1, 7 (range, 3‒11) in cohort 2, and 6 (range, 5‒8) in cohort 3. Only 3 patients remained in follow-up when the study was terminated by the sponsor because evaluation of the primary objective had been completed. Overall, 13 of 15 patients received subsequent anticancer therapy after discontinuing study treatment (Online Resource 1).
Fig. 1
Disposition of patients in the study. AE, adverse event
SafetyThree patients in cohort 1 experienced a DLT of grade 3 febrile neutropenia during cycle 1. One of these patients also experienced grade 4 laryngeal stenosis that was considered a DLT and discontinued from the study. The other 2 patients received filgrastim and meropenem or cefepime and were able to continue to cycle 2 without delay; the etoposide dose was reduced to 80 mg/m2 for both patients, and the cisplatin dose was reduced to 60 mg/m2 for 1 patient. No patients in cohort 2 or cohort 3 experienced a DLT.
All 15 patients receiving pembrolizumab in combination with platinum-etoposide chemotherapy experienced ≥ 1 treatment-related AE; the incidence of AEs was similar across all 3 cohorts (Table 2). Discontinuation due to treatment-related AEs was reported in 2 patients (1 each in cohort 1 and cohort 2). No AEs led to death. Serious treatment-related AEs were interstitial lung disease, febrile neutropenia, and laryngeal stenosis (n = 1 each) in cohort 1 and peripheral sensory neuropathy and lichenoid keratosis (n = 1 each) in cohort 2; no serious AEs were reported in cohort 3. Across all cohorts, the most frequently occurring treatment-related AEs included leukopenia, neutropenia, and anemia (Table 2). The most frequently occurring grade 3 or 4 treatment-related AEs were neutropenia, leukopenia, and febrile neutropenia (Table 2).
Table 2 Summary of AEs (ATS Population)Immune-mediated AEs were pneumonitis (n = 2) in cohort 1 and adrenal insufficiency, hyperthyroidism, and hypothyroidism (n = 1 each) in cohort 3 (Table 2). The only grade ≥ 3 immune-mediated AE was pneumonitis reported in cohort 1 (Table 2). No grade ≥ 3 immune-mediated AEs were reported in cohort 2 or cohort 3.
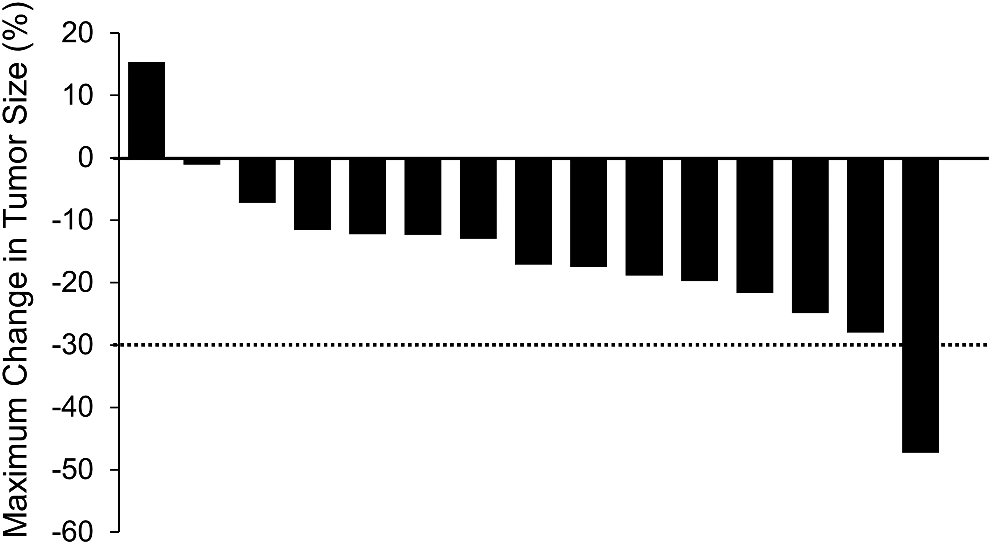
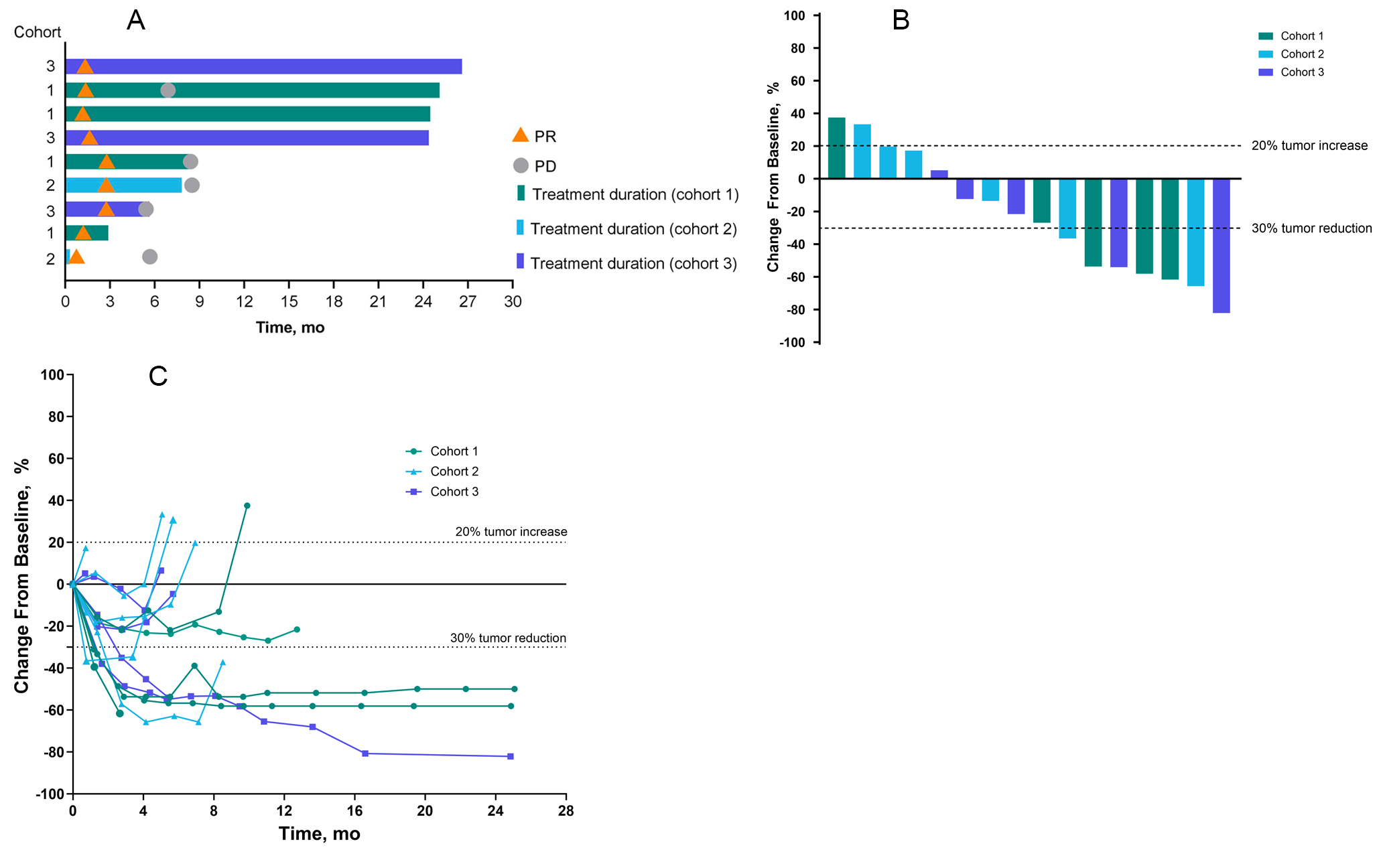
Antitumor activityThe ORR across all patients was 67% (95% CI, 38%‒88%). All 10 responses were PRs; no patient experienced a CR (Fig. 2A). The ORR was 50% (95% CI, 12%‒88%) in cohort 1, 83% (95% CI, 36%‒100%) in cohort 2, and 67% (95% CI, 9%‒99%) in cohort 3. Median time to response in all patients was 1.4 months (range, 1.2‒3.0 months) and median DOR was 4.5 months (range, 2.8‒28.8 months). Reductions in tumor size from baseline occurred in 14 of 15 patients (n = 8 in cohorts 1 and 3 combined and n = 6 in cohort 2; Fig. 2B, C).
Fig. 2
Survival and duration of response in individual patients (A), best change in sum of diameters of target lesions from baseline in individual patients (B), and percentage change in diameters of target lesions over time in individual patients (C). In panel A, bar lengths indicate follow-up duration. PD, progressive disease; PR, partial response; SD, stable disease
At the time of data cutoff, 14 of 15 patients (93%) had experienced a PFS event. Across all patients, median PFS was 4.2 months (95% CI, 3.0‒7.8 months), with an estimated PFS rate of 80% (95% CI, 50.0%‒93.1%) at 3 months and 40% (95% CI, 16.5%‒62.8%) at 6 months. Median PFS was 4.8 months (95% CI, 1.6 months‒not reached) for patients in cohort 1, 7.7 months (95% CI, 3.0‒30.2 months) for patients in cohort 2, and 4.2 months (95% CI, 3.9‒4.2 months) for patients in cohort 3.
Twelve of the 15 patients had died by the data cutoff date. Median OS among all patients was 22.1 months (95% CI, 7.4‒25.9 months), with an estimated 12-month survival rate of 53%. Median OS was 16.1 months (95% CI, 3.7 months‒not reached) in patients in cohort 1, 17.7 months (95% CI, 6.4 months‒not reached) in cohort 2, and 22.1 months (95% CI, 8.3 months‒not reached) in cohort 3.
DiscussionPembrolizumab in combination with platinum-etoposide chemotherapy was generally well tolerated and showed antitumor activity in Japanese patients with ES-SCLC. DLT rates were 20% (3/15); all patients with a DLT received pembrolizumab in combination with cisplatin and etoposide (ie, cohort 1). Furthermore, this AE profile was generally consistent with findings in a global population receiving pembrolizumab and etoposide combined with either carboplatin or cisplatin for SCLC [14]. As anticipated based on previous reports evaluating pembrolizumab as monotherapy in patients with recurrent or metastatic SCLC [13] or in combination with etoposide-platinum in patients with ES-SCLC [14], previous reports evaluating pembrolizumab, and the immune-mediated mechanism of action for pembrolizumab, immune-mediated AEs were observed, including pneumonitis, adrenal insufficiency, hyperthyroidism, and hypothyroidism. One event of grade 3 pneumonitis occurred in 1 patient in cohort 1; no other grade ≥ 3 immune-mediated AEs were observed.
In this study, the ORR among all patients was 67% (95% CI, 38%‒88%), with a median time to response of 1.4 months (range, 1.2‒3.0 months) and median DOR of 4.5 months (range, 2.8‒28.8 months). While comparison with other studies may be difficult because of the small sample size, these results were consistent with the KEYNOTE-604 study, in which the ORR was 71% (95% CI, 64%‒76%) in the pembrolizumab plus etoposide and platinum group [14]. Among the 15 patients included in the current analysis, nearly all experienced a reduction in tumor size from baseline. Median PFS was 4.2 months (95% CI, 3.0‒7.8 months) and median OS was 22.1 months (95% CI, 7.4‒25.9 months). In the global population enrolled in KEYNOTE-604, pembrolizumab in combination with etoposide and platinum resulted in a similar median PFS of 4.5 months (95% CI, 4.3‒5.4 months) and DOR of 4.2 months (range, 1.0+ to 26.0+ months). However, median OS was 10.8 months (95% CI, 9.2‒12.9 months) in KEYNOTE-604 [14] and thus was markedly shorter than the median OS of 22.1 months (95% CI, 7.4‒25.9 months) in KEYNOTE-011 part E. Results from KEYNOTE-011 part E support the hypothesis that the combination of immune checkpoint inhibitors with chemotherapy provides antitumor activity and can improve outcomes in patients with SCLC.
Limitations of the study include the small number of patients and open-label design. Despite these limitations, the results of this study suggest that the effects of pembrolizumab in a Japanese population are consistent with previous reports in global clinical studies of patients with ES-SCLC.
KEYNOTE-011 part E found that pembrolizumab in combination with platinum-etoposide therapy had manageable toxicity and demonstrated antitumor activity in a Japanese population with ES-SCLC. The current study provides encouraging evidence for immunotherapy targeting the PD-1 pathway in Japanese patients with ES-SCLC. Ongoing studies are evaluating pembrolizumab in combination with chemotherapy and other agents, such as olaparib in patients with limited-stage SCLC (NCT04624204) and as a coformulation with the anti‒T-cell immunoglobulin and ITIM domain inhibitor vibostolimab (TIGIT; NCT05224141), in patients with ES-SCLC.
留言 (0)