
記住我


Although evidence supports the effectiveness of specific virtual care technologies in specific care contexts,1 often these technologies are used less than intended to realize a desired outcome, or their use wanes over time.2, 3 Variations in uptake and use may attenuate the potential benefits of virtual care technologies. In alignment with the Veterans Health Administration (VHA) Office of Connected Care, we use the term “virtual care” to refer to health technologies intended to enhance the accessibility, capacity, quality, and experience of health care for Veterans, their families, and their caregivers, wherever they are geographically located. Examples of virtual care include but are not limited to telehealth services (e.g., synchronous video visits, asynchronous image delivery, remote patient monitoring), mobile health applications (apps), automated text message platforms, patient health portals (e.g., My HealtheVet), and wearable devices (e.g., activity trackers).
Engagement with virtual care technologies includes all of a user’s involvement with a specific technology, from uptake to sustained interactions.4,5,6 Without adequate digital access, one cannot engage with a virtual care technology, and without engagement, one cannot realize desired outcomes from the technology. We therefore define engagement as the decision to adopt and continue using a specific virtual care technology over time. Furthermore, it is important to recognize that what constitutes engagement can vary across different virtual care technologies.7 For example, a self-help app may be intended for active use over a defined period. In contrast, apps such as CBT-I Coach, an adjunct app to cognitive behavioral therapy for insomnia, are designed for use in tandem with a particular treatment.8 Similarly, an automated text messaging protocol may deliver a mix of motivational messages requiring only passive reading and occasional responses to assessment questions, while a chronic disease remote patient monitoring program may require daily interactions such as answering questions and submitting symptoms and vital sign information. Thus, “engagement” is a dynamic term that is best understood in relation to specific technologies and healthcare use cases.
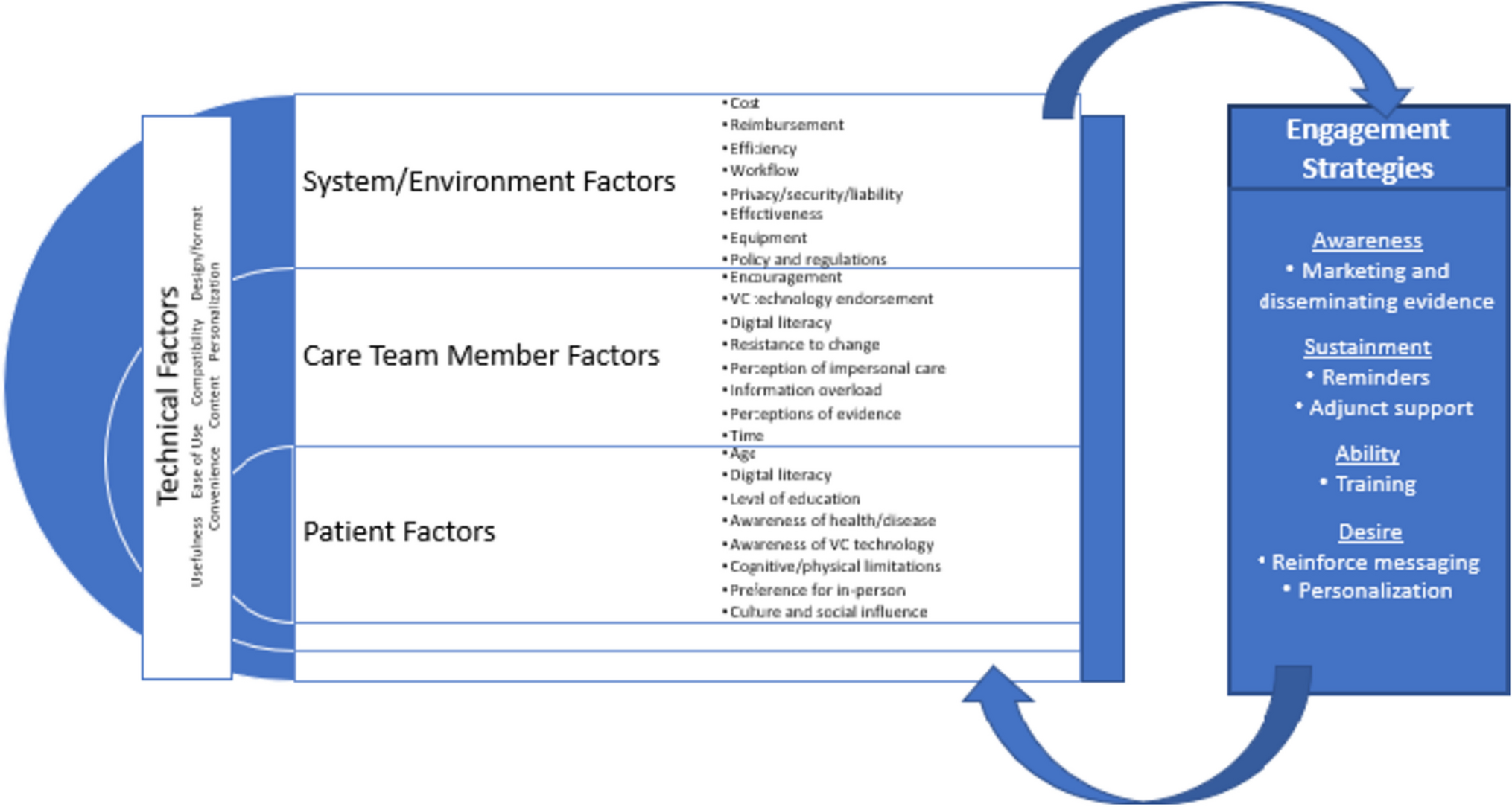
In Fig. 1, we introduce the Virtual Care Engagement Framework, which the present authors developed based on a review of the existing evidence. Factors at multiple levels can interact to influence Veteran virtual care engagement, including patient (e.g., age, health status/functioning, race, ethnicity, rurality),9,10,11,12,13 clinical team member (e.g., digital literacy, perceived burden, perceived value, proactive use of virtual care technologies),14,15,16,17 and system level factors (e.g., technology infrastructure, workflow, policy, and regulations).2, 15, 18, 19 Technical factors can vary by a technology or technology-assisted intervention itself, and may be cross cutting, requiring attention at different levels.20 Evaluating engagement is thus a complex endeavor. Strategies to increase virtual care engagement, such as adjunct support, training, and personalization, are designed to account for these factors. Conversely, some factors affect the use of these strategies depending on what is needed and who the strategy targets.
Figure 1
The virtual care engagement framework.
Healthcare organizations committed to the provision of high-quality virtual care, including VHA, have expressed the need for further investigation of these factors and of potential strategies that can be used to increase engagement. VHA’s Office of Connected Care (OCC) recognizes that the complex needs and risk factors of the Veteran population could impede Veteran engagement with virtual care technologies. In response, OCC designed and implemented various novel resources and innovative services across the VHA healthcare system to enhance engagement with virtual care technologies among different stakeholder groups. 21 These have included trainings, web-based video tutorials, help desk phone lines, toolkits, and Virtual Health Resource Centers within VHA facilities where Veterans and staff can receive training, hands-on support, and troubleshooting for use of different virtual care technologies.
Although increasing Veteran engagement with virtual care technologies is a VHA priority, research, clinical, and operations stakeholders lack consensus on a research agenda to support virtual care engagement and consequently, virtual care outcomes. Therefore, VHA Health Services Research & Development held a Virtual Care State of the Art (SOTA) Conference in May 2022 where separate workgroups convened to address research priorities for virtual care access, engagement, and outcomes. Here we report on findings from the engagement workgroup, including our workgroup processes, overarching workgroup discussion questions, key findings for each discussion question, and priorities for a research agenda on Veteran virtual care engagement in VHA.
留言 (0)