Study Design
This is a retrospective observational cohort study of PC VHA outpatient visits before the COVID-19 pandemic (March 1, 2019–February 28, 2020) and after the re-opening of VHA medical centers to in-person visits (October 1, 2020–September 30, 2021). Outpatient visits between March 1, 2020, through September 30, 2020, were excluded, because in-person restrictions dramatically decreased overall healthcare utilization and necessitated telemedicine use. VHA facilities lifted restrictions at varying times during the pandemic. This study followed the Strengthening the Reporting of Observational Studies in Epidemiology (STROBE) reporting guideline22and was approved by the University of Iowa Institutional Review Board and the Iowa City VA Healthcare System Research and Development Committee. It was conducted without direct patient contact using data routinely collected in the electronic health record. It was deemed of minimal risk; therefore, a waiver of informed consent was obtained.
Data Sources
Data were managed in the Veterans Informatics and Computing Infrastructure, a secure integrated system which includes all VHA administrative data and electronic health records. Patient-level data, including demographics, date, and delivery method for PC visits, as well as visits to the emergency department or urgent care, was obtained from the Corporate Data Warehouse (CDW) outpatient domain. The date of inpatient admissions was similarly identified using the CDW inpatient domain. The 2010 Census Bureau TIGER/Line shapefile contains geographic entity codes, including census block, census block group, and census tract. These data were spatially merged with the fiscal year-specific latitude and longitude of each veteran’s home address to identify their census block-based broadband availability using the December 2019 Federal Communications Commission (FCC) Fixed Broadband data,23 their census block group-based area deprivation index (ADI),24 a ranking of neighborhood socioeconomic disadvantage, and their census tract-based social vulnerability index (SVI),25 a Centers for Disease Control and Prevention measure of a community’s ability to respond to a hazardous event. Residential rurality classification was obtained from the Planning Systems Support Group (PSSG).
Patient Population
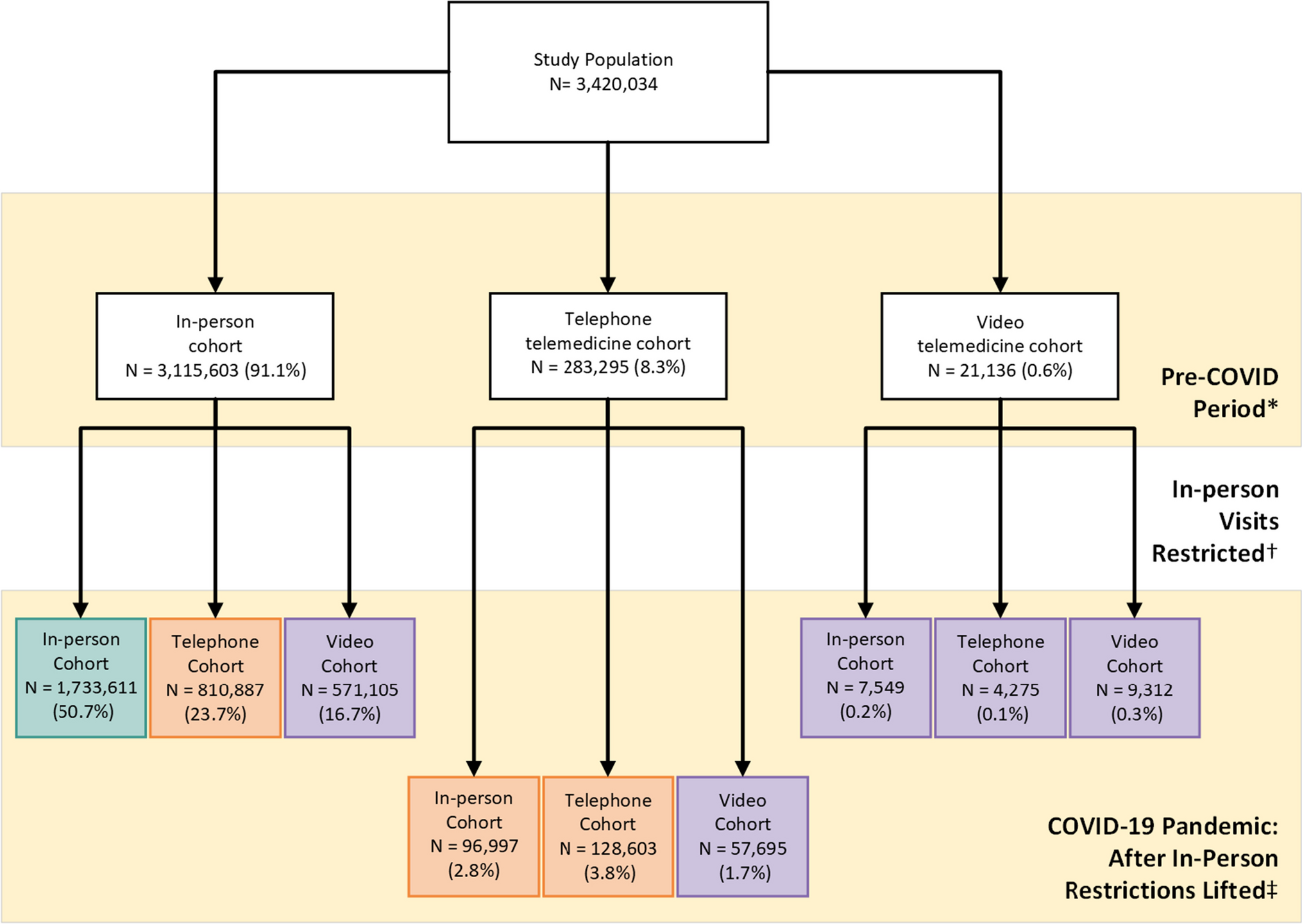
We established a cohort of veterans who used outpatient VHA PC prior to the pandemic (March 1, 2019–February 28, 2020) and after the re-opening of VHA medical centers (October 1, 2020–September 30, 2021). This ensured the comparison of healthcare utilization among the same group of veterans. PC encounters were categorized using stop codes, a pair of proprietary three-digit codes assigned to each outpatient encounter (Appendix 1). To be included, a veteran was required to have at least one PC visit, regardless of visit modality (i.e., in-person, telephone, or video) in each study period. We excluded care received at residential rehabilitation centers, nursing homes, or domiciliary.
Telemedicine Use
Our primary exposure was PC telemedicine (i.e., telephone or video) use. An index visit was the first PC visit within the study period, with each subsequent index visit occurring at least 7 days later. Index visits were not restricted by visit modality. Within the 7-day follow-up period, we assessed the number of days on which a PC visit occurred, categorized by visit modality (e.g., in-person, telephone, or video). Veterans were categorized into three mutually exclusive modality groups using index and intermediate PC visits throughout the study period overall as (1) in-person only, (2) telephone telemedicine (≥ 1 telephone visit with or without in-person visits), or (3) video telemedicine (≥ 1 video visit with or without telephone and/or in-person visits).
Outcomes
We studied three outcomes in the 7 days following an index PC visit: (1) emergent care (i.e., emergency department or urgent care visits), (2) any inpatient admission, and (3) any ACSC admission. Conditions included as ACSCs were community-acquired pneumonia, urinary tract infections, long- and short-term diabetes complications, lower-extremity amputation among diabetic patients, chronic obstructive pulmonary disease or asthma in older adults, heart failure, hypertension, and admission for asthma among young adults with diabetes.
Covariates
Patient demographics included age, sex, race, ethnicity, broadband availability, ADI, and SVI. Residential rurality was identified using the geocoded location of the patient’s home via Rural Urban Commuting Area codes and dichotomized into urban and rural (i.e., rural, highly rural, and insular categories).26 Race and ethnicity were self-reported. Race was categorized as American Indian/Alaska Native, Asian, Black/African American, Native Hawaiian/Pacific Islander, White, or Missing. Ethnicity was reported as being Hispanic, Not Hispanic, or Missing. Broadband availability was categorized according to download and upload speeds as inadequate (download ≤ 25 Mbps; upload ≤ 3 Mbps), adequate (download ≥ 25 Mbps and < 100 Mbps; upload ≥ 5 Mbps and < 100 Mbps), or optimal (download and upload ≥ 100Mbps). A minimum of 25 Mbps download and 3 Mbps upload are recommended for video telemedicine. We also calculated a comorbidity score based on the previous year using the methodology described by Quan et al. (2011), with a modification to allow for two outpatient diagnoses, as well as a single inpatient diagnosis.
Statistical Analyses
Demographic and healthcare utilization rates were compared to the in-person modality group (i.e., referent category) using chi-square or t-tests. Generalized estimating equations evaluated the difference in hospital utilization and PC visit modality group. The dependent binary variable indicated ever use of emergent care visit, any inpatient admission, or any ACSCs admissions, respectively, within 7 days of index PC visit. Independent variables included a binary indicator for study period (i.e., pre-pandemic vs. after in-person restrictions were lifted), a categorical variable for visit modality group, and their interaction. Odds ratios and 95% confidence intervals are reported for a model with and without the interaction term. Both models adjusted for patient characteristics and the number of intermediate PC visits within the 7-day follow-up window. All logistic regressions used the binomial model structure with a logit link function, an independent error structure, and standard errors clustered at the veteran level. All hypothesis tests were two-sided with an a priori 0.05 level of significance.
Sensitivity Analyses
Similar analyses considered a variety of follow-up windows from index visit (e.g., 3, 14, and 28 days), as well as the exclusion of any PC visit with a COVID-19 diagnosis.
The authors had full access to and take full responsibility for the integrity of the data. All analyses were conducted using SAS® statistical software version 9.2 (Cary, NC) and SQL Server Management, version 18.8.



留言 (0)