
記住我









The enzyme histone deacetylase type 6 (HDAC6) deacetylates α-tubulin, a component of microtubules that plays an important role in axonal transport. Despite its name, unlike other HDAC subtypes, it acts in the cytosol and not on histones.1,2 Histone deacetylase type 6 has been hypothesized to contribute to the pathophysiology of small fiber neuropathies such as painful diabetic peripheral neuropathy (DPN), chemotherapy-induced peripheral neuropathy (CIPN), and Charcot–Marie–Tooth disease (CMT).5 In rodent models of CIPN, HDAC6 inhibition and HDAC6 knockout are protective against loss of intraepithelial nerve fibers and mechanical allodynia,3,4 and HDAC6 inhibition can also reverse these findings after they have been induced.3 These results suggest that HDAC6 inhibition may have value as a treatment for DPN and CIPN and some subtypes of CMT.
The selective HDAC6 inhibitor ricolinostat is an orally administered investigational inhibitor of HDAC6 with a plasma half-life of approximately 4 hours. After administration of ricolinostat to humans, at exposures associated with the 120-mg dose of ricolinostat in the most current formulation, there is an approximately 4-fold increase in acetylated tubulin in peripheral blood mononuclear cells (PBMCs).6 We hypothesized that administration of ricolinostat to individuals with painful DPN could improve neuropathic pain and possibly other neuropathic signs and symptoms. To test this hypothesis, we conducted a 12-week, phase 2, randomized, double-blind, placebo-controlled study to assess of the efficacy of ricolinostat in individuals with painful DPN.
2. MethodsEligible subjects were 18 to 80 years with a documented history of type 1 or 2 diabetes for at least 6 months, hemoglobin A1c > 6.5% and <11%, and painful distal symmetric sensorimotor polyneuropathy because of diabetes defined as a Douleur Neuropathique (DN) score >4, moderate to severe pain, and one or more symmetric, distal neuropathic sign(s). Potentially confounding pain conditions were exclusionary, as was severe neuropathy, defined as a Utah Early Neuropathy Scale (UENS) score >24. Subjects taking a stable dose of duloxetine, gabapentin, pregabalin, or carbamazepine for >3 months could continue during the study. Other pain medications were not permitted, except acetaminophen 500 mg with a maximum of 2000 mg/d as needed.
Individuals meeting all above criteria and reporting average daily pain >4 and <9 on the 0- to 10-point numerical pain rating scale (NRS) with an SD <1.5 during the second week of a two-week lead-in observation phase were eligible to enter a 12-week, randomized, double-blind, treatment period with either ricolinostat 120 mg/d or matching placebo (1:1 randomization) followed by a 12-week open-label safety extension phase during which all participants received ricolinostat.
The protocol-specified primary outcome measure was mean change from baseline in average daily pain on the NRS self-reported in a daily diary. Secondary outcome measures included the change in UENS, the pain interference subscale of the Brief Pain Inventory Questionnaire (BPRS), the Patient Global Impression of Change (PGIC), the Neuropathy Total Symptom Score-6 (NTSS-6), and the Norfolk Diabetic Quality of Life-Diabetic Neuropathy (Norfolk Diabetic QOL-DN).
The planned sample of 274 patients was expected to provide 80% power to detect a group difference of 0.8 points on the NRS assuming an SD of 2.35. Patient treatment assignments were randomly generated by computer at Medpace, Inc (Medpace, Inc, Cincinnati, OH). Efficacy analyses included all randomized patients who received at least one dose of study drug with at least one postrandomization assessment, using mixed-model repeated-measures analysis for the NRS and ANCOVA for other measures assessed at baseline and endpoint only. Missing values for subjects who stopped treatment early were imputed using reference-based imputation based on the placebo group. Safety analyses included all subjects who received at least one dose of study drug.
The protocol was reviewed by a central or local institutional review board for each site in accordance with the Declaration of the World Medical Association. All subjects provided written informed consent to participate, and the study was listed on ClinicalTrials.gov (NCT03176472). Safety was reviewed during the study by an independent data monitoring committee.
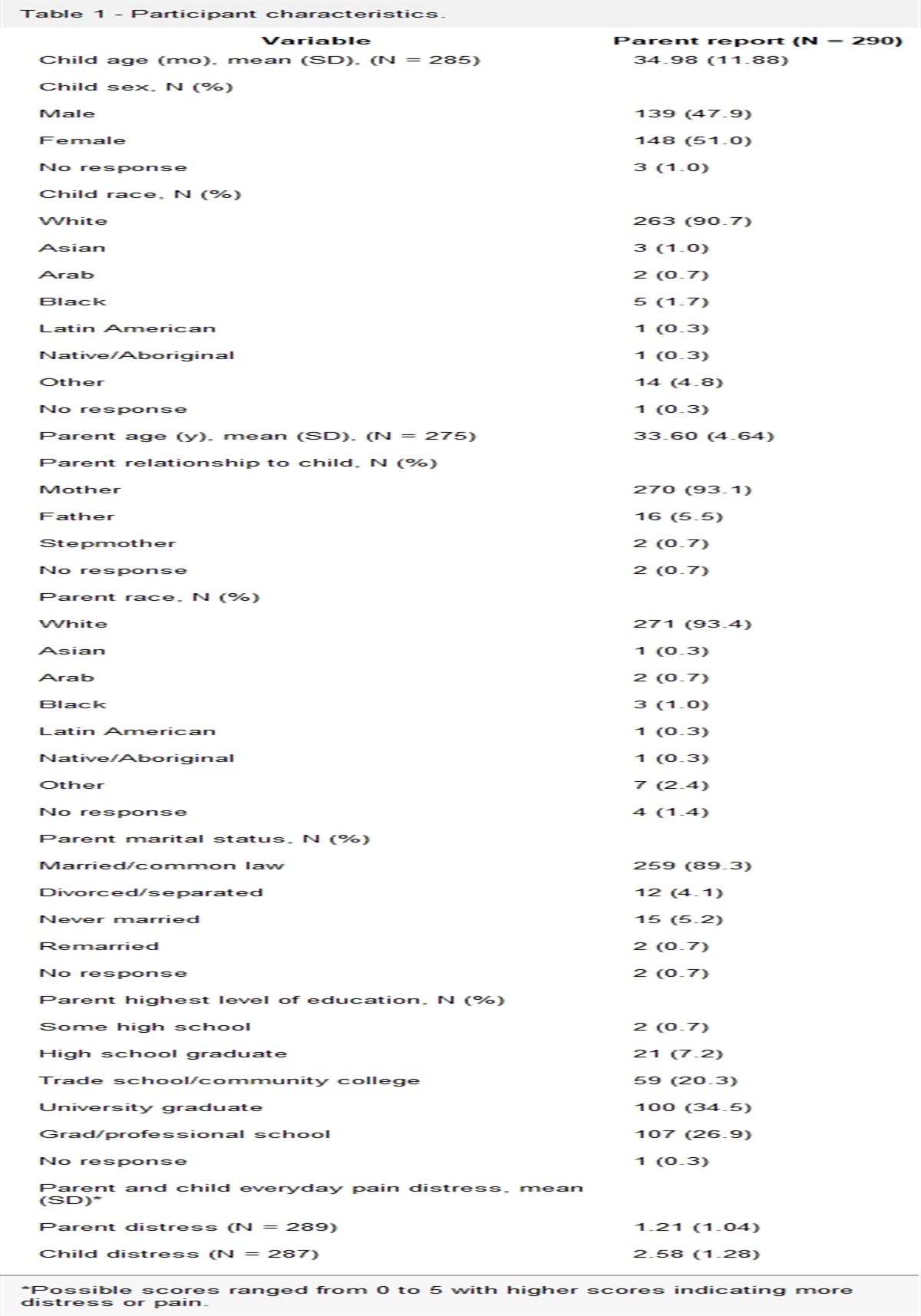
3. ResultsSubjects were enrolled at 32 investigative outpatient sites in the United States between December 2020 and January 2023. Of 1369 individuals screened, 569 met initial inclusion/exclusion criteria and entered the lead-in pain observation phase, of whom 282 met pain severity criteria and were randomized to either ricolinostat or placebo. The most common reasons for failure during the pain observation period were mild pain severity (N = 147), excessive pain variability (N = 48), and poor diary compliance (N = 37). Subject flow through the study is shown in the consort chart (Fig. 1). Subject demographics and characteristics were generally similar across the randomized groups (Table 1), as were routine laboratory measures. Medications for diabetes control were also similar across groups, with 62/140 (44%) of placebo and 50/142 (35%) of ricolinostat subjects continuing a permitted pain medication during the study. Baseline severity is shown in Table 2.
 Figure 1:
Figure 1: Consort chart.
Table 1 - Subject demographics and characteristics. Measure PlaceboDPN, diabetic peripheral neuropathy; HgbA1c, Hemolobin A1c.
BPRS, Brief Pain Inventory Questionnaire; NRS, numerical pain rating scale; NTSS-6, Neuropathy Total Symptom Score-6; QOL-DN, Quality Of Life-Diabetic Neuropathy; UENS, Utah Early Neuropathy Scale.
At 12 weeks, no significant differences between groups in change in pain severity or secondary measures were observed (Table 3). Additional change during the 12-week open-label extension was modest and similar in both groups (Table 3). Efficacy outcomes were not affected by baseline pain severity, concomitant pain medications, or other covariates. Safety and tolerability were generally good. Few discontinuations occurred as a result of adverse events. Treatment-emergent adverse events were experienced during the 12-week double-blind period by 52/140 (37%) of those on placebo and 53/142 (37%) on ricolinostat. Only 3 individual events were reported by more than 2% of the ricolinostat group: urinary tract infection (placebo 2/140, 1.4%; ricolinostat 5/142, 3.5%), nausea (placebo 5/140, 3.6%; ricolinostat 3/142, 2.1%), and diarrhea (placebo 8/140, 5.7%; ricolinostat 3/142, 2.1%). Among laboratory examinations during the 12-week period, 27/140 (19%) subjects on placebo and 38/142 (27%) on ricolinostat experienced reversible decreases from baseline in neutrophil counts >500 × 103/mm3 on 2 consecutive visits. The only subject with a decrease in neutrophil count below 1.25 × 103/mm3 was in the placebo group.
Table 3 - Outcomes at study endpoint. Results are LS mean (SE) except where indicated Placebo (N = 139) Ricolinostat (N = 141) P NRS change from baseline −1.0 (0.1) −1.2 (0.1) 0.38 Proportion of subjects with >30% NRS improvement at week 12 32/115 (28%) 44/124 (36%) 0.21 Proportion of subjects with >50% NRS improvement at week 12 16/115 (14%) 24/124 (19%) 0.30 UENS change from baseline −1.8 (0.4) −1.51 (0.4) 0.56 BPI-SF change from baseline −1.03 (0.2) −0.95 (0.2) 0.74 NTSS-6 change from baseline −2.3 (0.3) −2.1 (0.3) 0.72 Norfolk Diabetic QOL-DN change from baseline −7.8 (1.6) −7.6 (1.5) 0.93 PGIC-improvement endpoint score 3.2 (0.1) 3.2 (0.1) 0.54 Week 24 results (subjects who entered the open-label extension) Placebo-ricolinostat (N = 121) Ricolinostat-ricolinstat (N = 131) NRS mean (SE) change from baseline at week 24 −1.7 (0.2) −1.9 (0.2) UENS mean (SE) change from baseline at week 24 −2.2 (0.6) −1.5 (0.5)BPI-SF, Brief Pain Inventory Short Form; NRS, numerical pain rating scale; NTSS-6, Neuropathy Total Symptom Score-6; PGIC, Patient Global Impression of Change; QOL-DN, Quality Of Life-Diabetic Neuropathy; UENS, Utah Early Neuropathy Scale.
Ricolinostat did not improve neuropathic pain in individuals with DPN compared with placebo. These results do not support HDAC6 inhibition as an efficacious treatment for pain relief in people with established painful DPN or suggest that inhibition of HDAC6 over 12 weeks can reverse already established painful DPN. Ricolinostat was also not superior to placebo in reducing nonpain neuropathic signs as assessed by the UENS after 12 weeks.
Although these results do not support the use of ricolinostat in DPN, treatments that act to improve outcomes by restoring nerve function as hypothesized for ricolinostat may, particularly for nonpain aspects of neuropathy, require extended treatment times. Therefore, it is possible different results would be seen with longer treatment. Other factors could also have affected the observed outcomes. The study was sized based on a treatment difference of 0.8 points on the NRS, and the observed 0.2 difference may represent a true drug effect too small to be detected in this study, although the absence of a similar pattern on secondary efficacy measures argues against this. The favorable retention rate at 12 weeks, absence of serious safety concerns, and good study drug adherence as reported in study diaries suggest that study execution issues are unlikely to account for a failure to observe an effect on neuropathic pain. Although nonspecific (placebo) effects and variability can mask efficacy in pain studies, the relatively modest response in the placebo group and low variability in NRS scores (observed SD of 1.7 vs SD of 2.35 used for sample size calculation) make this unlikely.
This trial was designed and sized primarily to measure an effect on symptomatic neuropathic pain; however, an effect achieved through disease modification may require different design elements and, as noted above, would likely be difficult to observe in a 12-week study. The study did not define different sensory phenotypes using questionnaires or measures such as quantitative sensory testing, and the results do not exclude the possibility that specific subgroups not identified in this study could be responsive to HDAC6 inhibition. Another consideration is the degree and duration of HDAC6 inhibition. Administration of ricolinostat 120 mg to humans is associated with an approximately 4-fold increase in acetylated tubulin in PBMCs, but we have not measured tubulin acetylation within nerve axons. It is possible that less inhibition occurs in the axon or that greater inhibition or a longer time on target than that provided by the 4-hour half-life is necessary for a therapeutic benefit. However, as ricolinostat reaches an absorption limit at doses above 120 mg, we could not test the effect of greater inhibition.
In summary, HDAC6 inhibition with ricolinostat 120 mg daily for 12 weeks was not associated with a reduction in neuropathic pain compared with placebo in individuals with painful DPN. However, the results of this study suggest that selective HDAC6 inhibition has a favorable safety and tolerability profile and do not rule out the possibility of greater HDAC6 inhibition and/or studies of longer duration having symptomatic or disease-modifying benefits for DPN or other small fiber neuropathies such as CIPN or Charcot–Marie–Tooth disease.
DisclosuresD.M., W.C., S.J., M.J., M.H., and T.K. are employees or former employees (M.J.) of Regenacy Pharmaceuticals. R.F., R.D., D.H., R.P.-B., and R.M. are paid consultants to Regenacy Pharmaceuticals, and A.S. was a paid investigator in the study. J.V., M.J., T.V., and B.H. are employees of Medpace Inc.
AcknowledgementsThe study described here was funded by Regenacy Pharmaceuticals. The authors gratefully acknowledge the contributions of Medpace Inc, Analgesic Solutions, and Nathaniel Katz, MD, the investigators and participants in this study, and the members of the independent data monitoring committee, John Markman, MD, William Potter, MD, PhD, Chuck Davis, PhD, and Kirk Ways, MD, PhD.
Data availability: Because of commercial considerations, supporting data are not available at this time.
Funding was provided by Regenacy Pharmaceuticals, Inc.
References [1]. Badding M, Dean D. Highly acetylated tubulin permits enhanced interactions with and trafficking of plasmids along microtubules. Gene Ther 2013;20:616–24. [2]. Dompierre J, Godin J, Charrin B, Charrin BC, Cordelières FP, King SJ, Humbert S, Saudou F. Histone deacetylase 6 inhibition compensates for the transport deficit in Huntington's disease by increasing tubulin acetylation. J Neurosci 2007;27:3571–83. [3]. Krukowski K, Ma J, Golonzhka O, Laumet GO, Gutti T, van Duzer JH, Mazitschek R, Jarpe MB, Heijnen CJ, Kavelaars A. HDAC6 inhibition effectively reverses chemotherapy-induced peripheral neuropathy. PAIN 2017;158:1126–37. [4]. Ma J, Trinh R, Mahant I, Peng B, Matthias P, Heijnen C, Kavelaars A. Cell-specific role of histone deacetylase 6 in chemotherapy-induced mechanical allodynia and loss of intraepidermal nerve fibers. PAIN 2019;160:2877–90. [5]. Morfini G, Burns M, Binder L, Kanaan NM, LaPointe N, Bosco DA, Brown RH, Brown H, Tiwari A, Hayward L, Edgar J, Nave K-A, Garberrn J, Atagi Y, Song Y, Pigino G, Brady ST. Axonal transport defects in neurodegenerative diseases. J Neurosci 2009;29:12776–86. [6]. Yee AJ, Bensinger WI, Supko JG, Voorhees PM, Berdeja JG, Richardson PG, Libby EN, Wallace EE, Birrer NE, Burke JN, Tamang DL, Yang M, Jones SS, Wheeler CA, Markelewicz RJ, Raje NS. Ricolinostat plus lenalidomide, and dexamethasone in relapsed or refractory multiple myeloma: a multicentre phase 1b trial. Lancet Oncol 2016;17:1569–78.
留言 (0)