1. Introduction
Complex regional pain syndrome (CRPS) is a primary pain condition that is characterized by disproportional pain after an initiating noxious event such as trauma or surgery.28 Clinical manifestations are heterogenous and include sensory (allodynia, hyperpathia), vasomotor and sudomotor (temperature asymmetry, skin color changes, edema, sweating asymmetry), motor (decrease of range of motion, weakness, tremor, dystonia), and trophic changes of the hair, nails, and skin in the affected limb.28 Although favorable prognosis has been described in some,33 many patients develop chronic CRPS with persistent pain and functional disability.3
From its inception as a diagnostic term in 1994, CRPS was intended to serve as an umbrella diagnosis that encompassed a variety of painful disorders.40 In the past, several attempts have been made to classify this heterogenous condition into meaningful clinical subtypes. For example, the original 1994 diagnostic nomenclature specified 2 subtypes reflecting the previous distinction between older diagnoses of reflex sympathetic dystrophy and causalgia: CRPS type I (without major peripheral nerve damage) and CRPS type II (with major peripheral nerve damage), respectively.40 However, despite increasing research in the field of CRPS, current treatment regimens remain inadequate, and it is unclear whether the CRPS type I vs CRPS type II subtype distinction meaningfully affects treatment outcomes.8
It is possible that to date, the lack of significant efficacy in large pharmaceutical trials may arise because of the existence of multiple CRPS subtypes in trial samples selected based on current broad diagnostic criteria (eg, the new IASP criteria, formerly known as the Budapest criteria) that dilute beneficial treatment effects for a responsive patient subtype when grouped together. Different disease mechanisms may underlie different CRPS clinical phenotypes (ie, subtypes) and therefore may require different types of treatments.6 To develop more effective CRPS treatments, it is critical to identify relevant CRPS subtypes (ideally reflecting CRPS mechanisms) that specific treatments with known mechanisms of action can target (ie, precision medicine). Several subtypes have been proposed in the literature, but no systematic summary of the evidence is available. Hence, the aim of this review was to systematically identify and summarize the evidence for subtypes in CRPS.
2. Methods
This systematic review was conducted in accordance with the recommendations by the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA statement),45 and the study was registered in the Open Science Framework (https://osf.io).
2.1. Search strategy
We performed a comprehensive electronic search in MEDLINE (OvidSP), Embase (Elsevier), Cochrane, Scopus, and Web of Science from inception to July 2022 to identify relevant references. The terms for the search strategies were identified through discussion between an information specialist and the review team, by scanning the background literature and by browsing the MEDLINE Thesaurus (MeSH). The combinations of the following search keywords and MeSH terms were used in title, abstract and keywords: “reflex sympathetic dystrophy,” “complex regional pain syndrome,” ‘CRPS,” “algodystrophy,” “Sudeck” AND “subgroup,” “subtype,” “subset,” “phenotype,” “cluster.” The search was performed by a professional information specialist. To ensure the completeness of the literature search, 2 reviewers who were experienced clinicians and researchers in the field of CRPS screened bibliographies of all included studies and retrieved articles in an additional hand search. All potentially eligible references were included in the full-text review (inclusion criteria applied).
2.2. Study selection and main outcome variables
The eligibility criteria for inclusion in the current systematic review were (1) human studies, (2) established diagnosis of CRPS by applying disease-specific diagnostic criteria, and (3) reporting of at least one subtype (or subgroup, subset, phenotype or cluster) within a CRPS sample. We applied no language restriction. Opinion papers, letters, conference abstracts and review articles were excluded.
2.3. Risk of bias assessment
The quality of all studies was assessed using the MINORS criteria (methodological items for nonrandomized studies).48 These criteria assess 8 critical aspects of study design for noncomparative clinical studies and an additional 4 aspects of study design for comparative clinical studies. Each item is given a score of zero if information is not reported, one if information is reported but inadequate, and 2 if information is reported and adequate. The sum score results in a maximum score of 16 for noncomparative studies and 24 for comparative studies. Each score was then converted into a percentage to harmonize the scoring system. Depending on the score achieved, studies were qualified as either having low-risk of bias (≥75%), moderate-risk of bias (50% ≤ score <75%), or high-risk of bias (<50%).
2.4. Analysis
Citations from the initial search results of each database were exported to EndNote (version X9.2, Clarivate Analytics, Philadelphia, PA), and duplicates were removed. The titles and abstracts were screened and reviewed by 2 authors (L.K. and F.B.). Then, full texts of potential studies were retrieved and independently reviewed in detail for inclusion based on the predetermined criteria. Discrepancies between the 2 authors were resolved by discussion, and a third author (S.B.) was consulted if consensus could not be reached.
One author (F.B.) extracted the data from the included studies into a piloted standardized data collection form, and another author (L.K.) cross-checked the extracted data. The following data were extracted: author, year, study design, diagnostic criteria, number of participants with CRPS and their age, sex, site of CRPS, and disease duration. Subtypes were investigated or identified, and the main findings were also extracted.
3. Results
3.1. The flow of study selection
The search retrieved 8974 total records. With duplicates removed before screening, there were 4239 potentially relevant references. After screening titles and abstracts, the full text of 94 abstracts was reviewed. Of these, 74 references were excluded because they did not meet the inclusion criteria, leaving 20 included studies. Five additional studies were added based on the hand search.4,26,30,51,52 In total, 25 studies were included in the final analysis. Figure 1 provides the PRISMA flow diagram.
;) Figure 1.:
Figure 1.: Study selection according to the Preferred Reporting Items for Systematic Reviews and Meta-Analysis (PRISMA) flowchart.
3.2. Characteristics of the included studies and the patients
The characteristics of the studies and the patient samples for each are summarized in Table 1. The studies were published between 2002 and 2022. In the majority of studies, the diagnosis was based on the current International Association for the Study of Pain (Budapest) criteria (N = 16).1,4,9,13,18–23,25,30,38,39,55,57 Most studies employed a cross-sectional (N = 16)4,11,14,15,20,21,23,25,26,30,39,51–55 or cohort (N = 6)1,8,9,13,18,38 design. Some of the studies limited the inclusion to patients with CRPS type I (N = 8),8,11,30,51–55 and some studies did not report whether patients had CRPS type I or CRPS type II (N = 6).14,15,19,25,38,57 The majority of studies included patients with upper and lower extremity CRPS (N = 15).4,8,9,11,13–15,18,20,21,23,25,39,55,57 A total of 4908 patients (mean of 207 per study, range 37–1037) with a mean age of 46.9 years (SD 5.1) were included in the analysis. All studies predominantly included female participants (mean 68.5%) consistent with the sex difference previously noted in CRPS prevalence.12,46 The mean disease duration across studies ranged from 4 months4,25 to 9.3 years53 (mean, 2.9 years).
Table 1 -
Characteristics of the included studies.
Author, y (reference)
Study design
Diagnostic criteria
No. of participants with CRPS N, n
Age (y)
Female (%)
Site
Disease duration
Subgroups
Description
Alexander et al., 2012
1
Cluster analysis
IASP/Budapest
N = 148
CRPS type I: 100
CRPS-type II: 48
44.5 (range 20–68)
80
NR
8.8 y (range 0.7–36)
Two subgroups:
(1) Subgroup similar to healthy controls
(2) Subgroup with elevated levels of IL-1β, IL-4, IL-7, TNF-α, sIL-1RI, sIL-2Rα, sTNF-RI, sTNF-RII, IL-1Ra, and MCP-1
Evaluation of plasma levels of cytokines, chemokines, and their soluble receptors in CRPS patients vs gender-matched and age matched healthy controls
Significant changes were found in CRPS patients compared with healthy controls
Two clusters were identified in CRPS subjects
TNF-α was the most important category for cluster separation
When present, increased plasma levels of TNF-alpha correlated with disease duration and severity
Birklein et al., 2014
4
Cross sectional
IASP/Budapest
N = 55
CRPS type I: 44
CRPS type II: 11
49.8 (SEM 1.8, range 20–72)
67
UE, LE
16 wk (range 3–920)
Two subgroups:
(1) Acute CRPS (<3 mo)
(2) Chronic CRPS (>3 mo)
Detection of keratinocyte and mast cell proliferation in skin biopsies from the CRPS limb and the contralateral limb and identification of the cellular source of the upregulated TNF-alpha, IL-6, and tryptase
Epidermal thickness and keratinocyte expression were increased in acute CRPS skin and decreased in chronic CRPS skin. Increases in TNF-alpha and IL-6 immunostaining were more frequent in acute CRPS skin than in chronic CRPS skin. Tryptase-positive dermal mast cell numbers were also increased in acute CRPS skin but similar to contralateral skin in chronic CRPS skin. Numbers of tryptase-labelled mast cells correlated positively with temperature asymmetry (warm CRPS limb)
Bruehl et al., 2002
8
Cross sectional, cohort, cluster analysis
IASP/Orlando
N = 113
CRPS type I: 113
CRPS type II: 0
41.3 (SD 9.9)
62.5
UE, LE
26.9 mo (SD 28.8)
Three subgroups:
(1) Vasomotor subgroup
(2) Neuropathic/sensory abnormalities subgroup
(3) Florid CRPS subgroup
Cluster analysis based on signs and symptoms of the diagnostic criteria resulted in the 3 subgroups
Identified subgroups did not differ significantly regarding pain duration. Rate of abnormalities on EMG/nerve conduction studies was most common in the neuropathic/sensory abnormalities subgroup
Bruehl et al., 2016
9
Prospective, between-subject, and within-subject design, 3 mo follow-up, cluster analysis
IASP/Budapest
N = 152
CRPS type I: 129
CRPS type II2: 23
46.4 (SD 13.4)
74.2
UE, LE
4.7 mo (warm CRPS)
20 mo (cold CRPS)
Two subgroups:
(1) Warm CRPS
(2) Cold CRPS
Cluster analysis based on signs and symptoms of inflammation resulted in the 2 subgroups
Subgroups did not differ significantly regarding pain intensity
Pain duration was shorter in warm CRPS (4.7 mo) than in cold CRPS (20 mo). Inflammatory score was elevated in warm CRPS and decreased over the 3-mo follow-up in warm CRPS but did not change in cold CRPS
De Boer et al., 2011
11
Cross sectional
IASP/Orlando
N = 681
CRPS type I: 681
CRPS type II: 0
47.2 (SD 13.8)
82.8
UE, LE
14.4 (IQR 3.6–73.2)
Four subgroups based on disease duration:
(1) <2 mo
(2) 2–6 mo
(3) 6–12 mo
(4) >12 mo
Description and assessments of signs and symptoms in relation to disease duration
Sensory signs (allodynia, hyperalgesia) and motor signs (except limited range of motion) occurred more in patients with a longer disease duration (>6 mo) than in patients with a shorter disease duration
Vasomotor and sudomotor signs were less frequent in patients with longer duration (>6 mo)
Changes in nail growth (but not skin or hair growth) were more frequent in patients with longer disease duration
De Mos et al., 2009
13
Cluster analysis
IASP/Budapest
N = 102
CRPS type I: 99
CRPS type II: 3
51 (12–86)
79
UE, LE
5.8 y (range: 2.1–10.8)
Three subgroups:
(1) Best-outcome subgroup
(2) Moderate-outcome subgroup
(3) Poor-outcome subgroup
Retrospective analysis of electronic patient records with CRPS patients and reference patients with an identical past injury but without CRPS.
Patients with poor outcome more often had cold upper extremity CRPS with initiating event other than fracture. Disease duration did not differ between the groups
More patients in the poor-outcome group (based on the number of signs and symptoms) reported ongoing disease progression, ongoing treatment, and poorer work status
De Rooij et al., 2009
14
Cross sectional
IASP/Orlando
N = 271
CRPS type I: NR
CRPS type II: NR
36.7 (SD 14.5)
83
UE, LE
NR
Two subgroups:
(1) Familial CRPS subgroup
(2) Sporadic CRPS subgroup
Evaluation of familial occurrence in CRPS patients
Familial CRPS patients had younger age at onset, multiple affected extremities, dystonia
De Rooij et al., 2010
15
Cross sectional
IASP/Orlando
N = 537
CRPS type I: NR
CRPS type II: NR
42.5 (SD 15.6)
78
UE, LE
1.1 y (IQR 0.3–2.8)
Two subgroups:
(1) Spontaneous onset of CRPS
(2) Trauma-induced onset of CRPS
Comparison of phenotypic characteristics of patients with spontaneous and trauma-induced CRPS
Patients with spontaneous onset were younger at onset and had a longer disease duration. Clinical presentation was similar in the 2 groups
Dimova et al., 2020
18
Cluster analysis
IASP/Budapest (research criteria)
N = 1037
CRPS type I: 890
CRPS type II: 147
51.7 (SD 13.1)
72.5
UE, LE
9.4 mo (SD 15.8)
Three subgroups:
(1) Peripheral inflammation phenotype
(2) Central phenotype
(3) Mixed phenotype
Cluster analysis of CRPS signs resulted in the 3 subgroups
The phenotypes may reflect major pathophysiologic mechanisms of peripheral inflammation and central changes
The 3 subgroups did not differ in relation to age, CRPS duration, sex, or CRPS type I or II
Dirckx et al., 2015
19
Retrospective
IASP/Budapest
N = 48
CRPS type I: NR
CRPS type II: NR
47.8 (SD 10.0)
66.7
NR
6 mo (IQR 12.75)
Three subgroups:
(1) Warm CRPS (ΔT ≥ 0.60°C in CRPS limb vs healthy limb)
(2) Cold CRPS (ΔT ≥ 0.60°C lower in CRPS limb vs healthy limb)
(3) Intermediate CRPS (neither cold nor warm)
Assessment of signs of inflammation in warm, cold, and intermediate CRPS
No difference in TNF-alpha and IL-6 in artificial skin blisters on the affected and nonaffected sides
Longer CRPS duration and lower age in cold CRPS than in warm CRPS
Cold CRPS and intermediate CRPS more often had signs of allodynia
Drummond et al., 2014
20
Cross sectional
IASP/Budapest
N = 37
CRPS type I: 29
CRPS type II: 8
47.2 (SD 11.1)
78.3
UE, LE
52.7 mo (SD 58.8)
Chronic CRPS (pain duration = 66 ± 14 mo)
To determine whether a central disturbance in somatosensory processing contributes to limb pain in CRPS.
Increase of pain in the CRPS limb when ipsilateral forehead was cooled in a subgroup with a longer pain duration and more pain in the CRPS limb
Drummond et al., 2018
21
Cross sectional
IASP/Budapest (research criteria)
N = 104
CRPS type I: 71
CRPS type II: 33
46.8 (SD 11.2)
70.2
UE, LE
49.0 mo (SD 27.0)
Two subgroup analyses (A, B)
(A) 2 subgroups:
(1) CRPS type I
(2) CRPS type II
and
(B) 3 subgroups:
(1) Acute CRPS (<12 mo)
(2) Intermediate CRPS (13–36 mo)
(3) Chronic CRPS (>36 mo)
Assessing hemisensory disturbances in CRPS patients
Increase in sharpness ratings to repeated pinprick was greater in the ipsilateral than in contralateral forehead in chronic but not in intermediate and acute CRPS
Patients with chronic CRPS were more sensitive to thermal stimuli on both sides of their body than patients with acute or intermediate CRPS
Cold-pain ratings were greater on the ipsilateral than on the contralateral side of the forehead in patients with chronic CRPS but not in patients with acute or intermediate CRPS
Tactile detection threshold to graded von Frey hairs was elevated in the CRPS 2 limb compared with contralateral limb but was similar in the affected and contralateral limb of patients with CRPS type I
Also, sensitivity to pinprick was lower in the CRPS limb of CRPS type II than in the CRPS type I patients
Brush-evoked allodynia was more common in the CRPS type II limb than in the CRPS type I limb
Patients with chronic CRPS type I more often had pressure-pain sensitivity and allodynia in the uninjured limb on the symptomatic side of the body than in patients with chronic CRPS type II
Drummond et al., 2018
22
Double-blind crossover trial
IASP/Budapest (research criteria)
N = 90
CRPS type I: 59
CRPS type II: 31
47.1 (SD 11.3)
70
UE
52 mo (SD 70 mo)
Three subgroup analyses (A, B, C)
(A) 2 subgroups
(1) Warm CRPS (≥1.0°C higher in CRPS limb vs healthy limb)
(2) Cold CRPS (≥1.0°C lower in CRPS limb vs healthy limb)
and
(B) 3 subgroups:
(1) Acute CRPS (<12 mo)
(2) Intermediate CRPS (13–36 mo)
(3) Chronic CRPS (>36 mo)
and
(C) 2 subgroups:
(1) CRPS type I
(2) CRPS type II
To evaluate whether upregulated cutaneous expression of α1-adrenoceptors is a source of pain in CRPS
Skin biopsies of the CRPS limb and the contralateral limb were assessed for adrenoceptors
Evoked pain and responses to pinprick was investigated to intradermal injections of α1-adrenoceptor agonist phenylephrine or α2-AR agonist clonidine in the CRPS limb and the contralateral limb
No differences were seen between thermal groups
α1-AR immunoreactivity was greater in nerve bundles bilaterally in CRPS patients than in controls and was greater in dermal nerves in the CRPS limb vs contralateral limb irrespective of CRPS duration. However, α1-AR immunoreactivity was greater in nerve bundles of the CRPS limb in patients with acute than intermediate or chronic CRPS but similar across duration in the contralateral limb
There was greater α1-AR immunoreactivity in nerve bundles of the CRPS 2 limb than in those of the CRPS type I limb. Greater α1-AR immunoreactivity was also seen in blood vessels in both limbs of CRPS type II than in the limbs of CRPS type I patients
A difference in α1-AR immunoreactivity in the epidermis was seen with disease duration in CRPS type I and type II. For CRPS type II, it was greater bilaterally in acute and intermediate vs chronic, but the opposite was seen in CRPS type I
A group of phenylephrine responders emerged across subgroups who became more sensitive to pinprick and had greater α1-AR in dermal nerve bundles
Eberle et al., 2009
23
Cross sectional
IASP/Budapest
N = 50
CRPS type I: 46
CRPS type II: 4
46.0 (SD 9)
92
UE, LE
21.5 wk (SD 3.0)
Two subgroups:
(1) Warm CRPS (mean ΔT = +1.0° in CRPS limb vs healthy limb)
(2) Cold CRPS (mean ΔT = −1.0°C in CRPS limb vs healthy limb)
Investigation of clinical differences in warm and cold CRPS
Cold CRPS patients more often reported a history of serious life events, chronic pain disorders, dystonia, cold-induced pain, and sensory loss to QST
Warm CRPS was characterized by mechanical hyperalgesia
Escolano et al., 2021
25
Cross sectional
IASP/Budapest
N = 38
CRPS type I: NR
CRPS type II: NR
48.0
62.3
UE, LE
16.9 wk
MMP-2
MMP-9
Comparison of MMP-2 and MMP-9 concentrations in skin and serum of patients with CRPS, other pain diseases, and healthy subjects
Low ipsilateral MMP-2 was associated with trophic changes
Contralateral MMP-2 was associated inversely with CRPS severity
Higher MMP-9 was associated with higher CRPS severity
Gierthmühlen et al., 2012
26
Cross sectional
IASP/Orlando and IASP/Budapest
N = 344
CRPS type I: 298
CRPS type II: 46
52.7 (SD 12.7)
78.8
UE
23.2 (SD 34.4)
Two subgroups:
(1) CRPS type I
2) CRPS type II
To investigate somatosensory signs in CRPS type I, CRPS type II, and peripheral nerve injury using QST
CRPS types I and II had similar somatosensory profiles in terms of hyperalgesia, allodynia, and thermal detection thresholds, but a loss of mechanical detection was more frequent in CRPS type II. Pressure hyperalgesia was most frequent in both CRPS types I and II compared with peripheral nerve injury. Hyperalgesia/allodynia without the loss of detection (only gain) was more common in CRPS type I than in CRPS type II. Correlations with symptom duration were mild. Small fiber deficits were less frequent than large fiber deficits
Huge et al., 2008
30
Cross sectional
IASP/Budapest (research criteria)
N = 65
CRPS-type I: 65
CRPS-type II: 0
59.1 (SD 12.9)
88.5
UE
22.4 (SD 20.4)
Two subgroups:
(1) Acute CRPS (≤12 mo)
(2) Chronic CRPS (>12 mo)
Investigation of thermal QST in acute and chronic CRPS patients vs a group of gender-matched and age-matched healthy controls
Patients with acute CRPS experienced warm and cold hyperalgesia and warm and cold hypoesthesia in the CRPS limb. Thermal hyperalgesia was lower in chronic CRPS, and warm and cold hypoesthesia was worse in chronic than in acute CRPS. Only patients with acute CRPS had paradoxical heat sensations. All QST changes were somewhat present in the contralateral limb
Patients with chronic CRPS had a cold CRPS limb and patients with acute CRPS a warm CRPS limb
Libon et al., 2010
38
Cluster analysis
IASP/Budapest (research criteria)
N = 137
CRPS type I: NR
CRPS type II: NR
43.8 (SD 11.9)
77.9
NR
NR
Three subgroups based on cognitive function:
(1) Normal
(2) Dysexecutive
(3) Global dysfunction
To elucidate the existence of neuropsychological subtypes using tests that assess executive control, naming/lexical retrieval, and declarative memory. Limb pain and depression were also assessed
Cognitive function subgroups did not differ in level of pain, CRPS duration, medication use, or number of limbs with CRPS. Neuropsychological variables did not covary with depression
Lunden et al., 2022
39
Cross sectional
IASP/Orlando and IASP/Budapest
N = 61
CRPS type I: 43
CRPS type II: 18
38.7 (spread not reported)
45.9
UE, LE
5 y (spread not reported)
Three subgroups:
(1) Thermal allodynia
(2) Thermal hyposensitivity
(3) Thermal allodynia und hyposensitivity
Investigation of whether the 3 QST subgroups differ with respect to limb pain characteristics
Paroxysmal pain (sudden stimulus–independent electric shock–like pain) was more prevalent in patients with thermal allodynia than in patients without allodynia
No difference between CRPS type I and type II
Van Rooijen et al., 2012
53
Cross sectional
IASP/Orlando (CRPS 1 with dystonia) and IASP/Budapest (research criteria) (CRPS 1 without dystonia)
N = 281
CRPS type I: 281
CRPS type II: 0
44.5 (SD 12.5)
59.4
NR
5.5 y (IQR 6.5–9.8)
Two subgroups:
(1) With dystonia
(2) Without dystonia
To test the genetic association with HLA-B62 and HLA-DQ8 in CRPS patients
CRPS with and CRPS without dystonia may be genetically different but overlapping disease entities because only HLA-DQ8 is associated with both
Van Rooijen et al., 2013
51
Cross sectional
IASP/Orlando
N = 48
CRPS type I: 48
CRPS type II: 0
46.7 (SD 12.1)
72.9
UE
9.3 y (IQR 3.5–14.7)
Two subgroups:
(1) With dystonia
(2) Without dystonia
To compare sensory function using QST between patients with dystonia, without dystonia, and healthy controls and to compare sensory functions with motor performance
Both patients with and without dystonia had a loss of function to warmth detection, cold detection, and a gain of function to cold pain and pressure pain in the CRPS limb
In addition, patients with dystonia experienced a loss of function for vibration detection and 2-point discrimination had a greater gain of function for pressure pain than patients without dystonia
Patients with dystonia were slower at recognizing their affected limb than those without dystonia and had poorer finger tapping performance than those without dystonia. Pressure-pain thresholds correlated with performance on finger tapping in all 3 groups and with dystonia severity
Van Rooijen et al., 2013
52
Cross sectional
IASP/Orlando
N = 48
CRPS type I: 48
CRPS type II: 0
46.4 (SD 12.1)
72.9
UE
10.0 (SD 7.4)
Two subgroups:
(1) With dystonia
(2) Without dystonia
To investigate sensory function using QST in unaffected limbs and cheeks of CRPS patients with and without dystonia and compare them with healthy controls
Pressure hyperalgesia was the most prominent finding at all unaffected sites in both patients with and without dystonia. Patients with and without dystonia were similar apart from a lower vibration threshold in patients with dystonia
Vaneker et al., 2005
54
Cross sectional
Veldman
N = 47
CRPS type I: 47
CRPS type II: 0
58 (SD 15)
70
UE
NR
Two subgroups:
1) Warm CRPS (mean ΔT = +0.65 in CRPS limb vs healthy limb)
(2) Cold CRPS (mean ΔT = −0.78°C in CRPS limb vs healthy limb)
To identify altered patterns of sensory processing using QST 8 y after diagnosis, to document differences in sensory processing between warm and cold CRPS, and to determine relationships between changes in sensory processing and disease progression regarding pain
Patients with cold CRPS had poorer clinical pain outcome, and more signs of central sensitization which increased with disease progression. Pressure-pain thresholds were lower in the CRPS limb in both groups and with disease progression
Varenna et al., 2016
55
Cross sectional
IASP/Budapest (research criteria)
N = 194
CRPS type I: 194
CRPS type II: 0
57.1 (SD 12.9)
62.9
UE, LE
4 mo (range 2–6)
Two subgroups:
(1) Warm CRPS
(2) Cold CRPS
Definition of warm vs cold not reported
To assess whether the effectiveness of bisphosphonates in CRPS patients is influenced by variables related to patient and/or disease characteristics
Responsiveness to bisphosphonates was predicted by warm disease subtype, shorter CRPS duration, and fracture as initiating event
Zyluk et al., 2013
57
Observational (registry)
IASP/Budapest
N = 220
CRPS type I: NR
CRPS type II: NR
NR
NR
UE, LE
NR
Three subgroups:
(1) Acute CRPS
(2) Chronic CRPS
(3) Chronic, refractory CRPS
Analysis of institutional CRPS register with particular attention to a chronic, refractory CRPS subtype that is extremely severe, has a disabling course, and is resistant to treatment
All patients with chronic refractory CRPS were female, and all experienced neurological symptoms (hyperpathia, allodynia, tremor, muscle cramps, dystonia)
AR, adrenoreceptor; CRPS, complex regional pain syndrome; HLA, human leucocyte antigen; IASP, International Association for the Study of Pain; IL, interleukin; LE, lower extremity; MMP, metallproteinase; NR, not reported; PTSD, posttraumatic stress syndrome; QST, quantitative sensory testing; TNF, tumor necrosis factor; UE, upper extremity; ΔT, temperature difference.
3.3. Quality assessment
All included studies were nonrandomized, which allowed the use of the MINORS criteria for quality assessment. Scores averaged 69.3% (range, 37.5%–83.3%). Of the 25 studies included, 16 were classified as having low risk of bias,1,4,9,11,13,18,21–23,25,26,30,51–54 8 studies with a moderate risk of bias,8,14,15,19,20,38,39,55 and 1 study with high risk of bias57 (Table 2).
Table 2 -
Individual risk of bias assessment using the methodological items for nonrandomized studies criteria.
Author, year (reference)
Clearly stated aim
Inclusion of consecutive patients
Prospective data collection
Endpoints appropriate to study aim
Unbiased assessment of study endpoint
Follow-up period appropriate to study aim
<5% loss to follow-up
Prospective calculation of study size
Adequate control group
Contemporary groups
Baseline equivalent groups
Adequate statistical analysis
Total score (%)
Risk of bias
Alexander et al., 2012
1
2
1
2
2
1
2
0
2
2
2
2
2
83.3%
Low
Birklein et al., 2014
4
2
1
2
2
2
2
0
0
2
2
2
2
79.2%
Low
Bruehl et al., 2002
8
2
1
2
2
0
2
0
0
NA
NA
NA
NA
56.3%
Moderate
Bruehl et al., 2016
9
2
1
2
2
2
2
1
0
NA
NA
NA
NA
75.0%
Low
De Boer et al., 2011
11
2
2
2
2
0
2
2
0
N/A
N/A
N/A
NA
75.0%
Low
De Mos et al., 2009
13
2
0
2
2
0
2
1
0
2
2
2
2
70.8%
Low
De Rooij et al., 2009
14
2
0
2
2
0
2
0
2
2
1
1
2
66.7%
Moderate
De Rooij et al., 2010
15
2
0
0
2
1
2
0
0
2
2
0
2
54.2%
Moderate
Dimova et al., 2020
18
2
2
2
2
2
2
0
0
NA
NA
NA
NA
75.0%
Low
Dirckx et al., 2015
19
2
0
0
2
2
2
0
0
2
2
0
2
58.3%
Moderate
Drummond et al., 2014
20
2
0
2
2
1
2
0
0
2



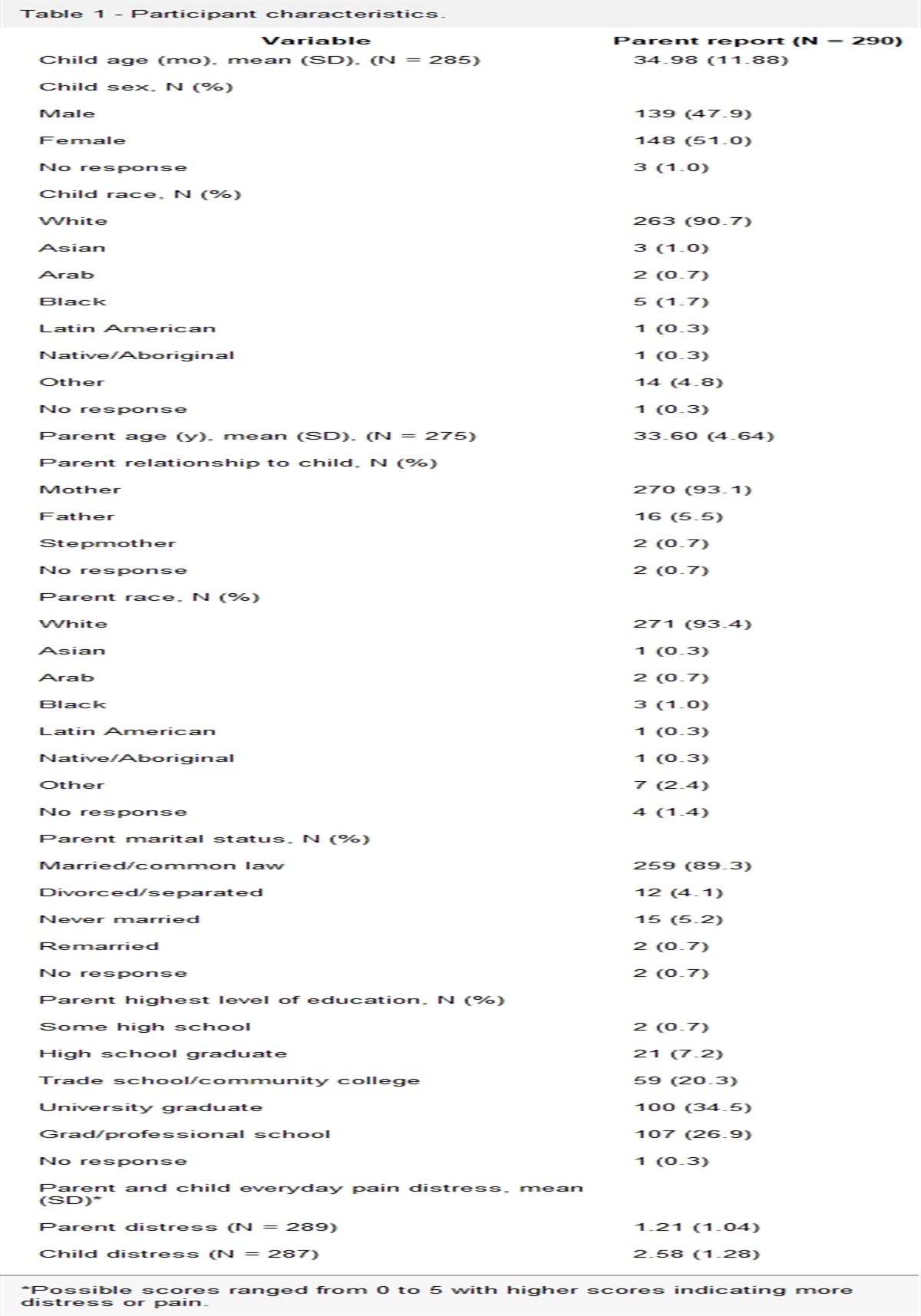







 Figure 1.:
Figure 1.:
Comments (0)