
記住我









Trigeminal neuralgia (TN) is a debilitating neuropathic facial pain disorder characterized by unilateral, recurrent, severe electric shock-like pains, abrupt in onset and termination, limited to the sensory distribution of one or more divisions of the trigeminal nerve, and triggered by innocuous stimuli.22 Trigeminal neuralgia is subclassified into: classical TN, developing without apparent cause other than neurovascular compression (NVC) of the trigeminal nerve root entry zone (TREZ) and frequently treated with surgical microvascular decompression (MVD); secondary TN, caused by an underlying disease (eg, multiple sclerosis [MS] or brain tumor); and idiopathic TN, occurring in the absence of NVC or another underlying lesion. Although pain symptoms are similar across TN categories, to date, no universal pathophysiological features of the disease have conclusively been identified. Brain MRI studies suggest that morphological changes to the TREZ occur on the symptomatic side in classical TN, with diffusion tensor imaging (DTI) studies in particular showing disruptions to trigeminal nerve microstructure, presumably by dysmyelination or demyelination.4,19,23,29 The TREZ is where the trigeminal nerve enters the brainstem and represents a transition zone from peripheral Schwann cell–mediated myelination to central oligodendrocyte-mediated myelination, making the area susceptible to pressure-induced lesions.20,38 Biopsies of the TREZ taken during surgery show axonal loss, axonal degradation, demyelination, and collagen deposition.24,41 Additionally, DTI studies in idiopathic TN found that nerve microstructural abnormalities exist irrespective of NVC.17,50 This may imply that neuroinflammation could be a common pathophysiological factor causing trigeminal nerve injury and contributing to the development of TN.6,17,50
Cerebrospinal fluid (CSF) regulates electrolyte balance, circulates active molecules, and eliminates catabolites in the neuronal environment.43 Cerebrospinal fluid protein alterations in disease reflect involvement of various biological pathways in disease pathophysiology.49 Early TN CSF studies focused primarily on neurotransmitters and neuropeptides,21 finding neurochemical changes including decreased norepinephrine and somatostatin, and increased substance P and neuropeptide Y (NPY).5,21,45 Ericson et al.18 identified significant increases in 21 inflammatory-related proteins in patients with TN compared with healthy controls, which appeared to normalize after successful MVD surgery. Abu Hamdeh et al.1 identified significant increases in apolipoproteins and proteins involved in the complement cascade in TN patients compared with control participants undergoing minor urological surgery. They also found that patients with TN exhibited increased CSF markers of peripheral demyelinating injury, immune tolerance, myelin destruction, neuronal cell death, and myelin clearance.46 These studies highlight the utility of further examining CSF inflammatory markers in TN to better understand the mechanisms underlying initiation and maintenance of pain in TN.
We therefore assessed the inflammatory profile of CSF in a cohort of TN patients undergoing MVD surgery compared with a pain-free control group, hypothesizing that there would be increased levels of CSF inflammatory markers in the former. Uniquely, we examined CSF immediately bathing the trigeminal nerve in the cerebellopontine angle cistern, as opposed to CSF collected through distant lumbar puncture.
2. Material and methods 2.1. Ethical approvalThis study received ethical approval from the Health Research Ethics Board of the University of Alberta.
2.2. Inclusion/exclusion criteriaPatients with TN were eligible for this study if they fit the following inclusion criteria: adult patients (18–80 years, male or female) with a confirmed TN diagnosis, preoperative MRI evidence of NVC, and who had provided informed consent to undergo MVD for surgical treatment of TN. Microvascular decompression is a surgical treatment option in medically refractory patients with classical TN that aims to resolve neurovascular compression (NVC) at the trigeminal nerve root by separating offending blood vessels from the trigeminal nerve.8 Control participants were eligible for this study if they matched the following inclusion criteria: adult patients (18–80 years, male or female) admitted to hospital for reasons other than TN and either (1) having in place a lumbar drain or (2) undergoing MVD surgery for a non-TN condition (eg, hemifacial spasm) as part of their care. Patients were ineligible for this study if they had a concurrent chronic pain condition or if their CSF was being analyzed for concern of infection.
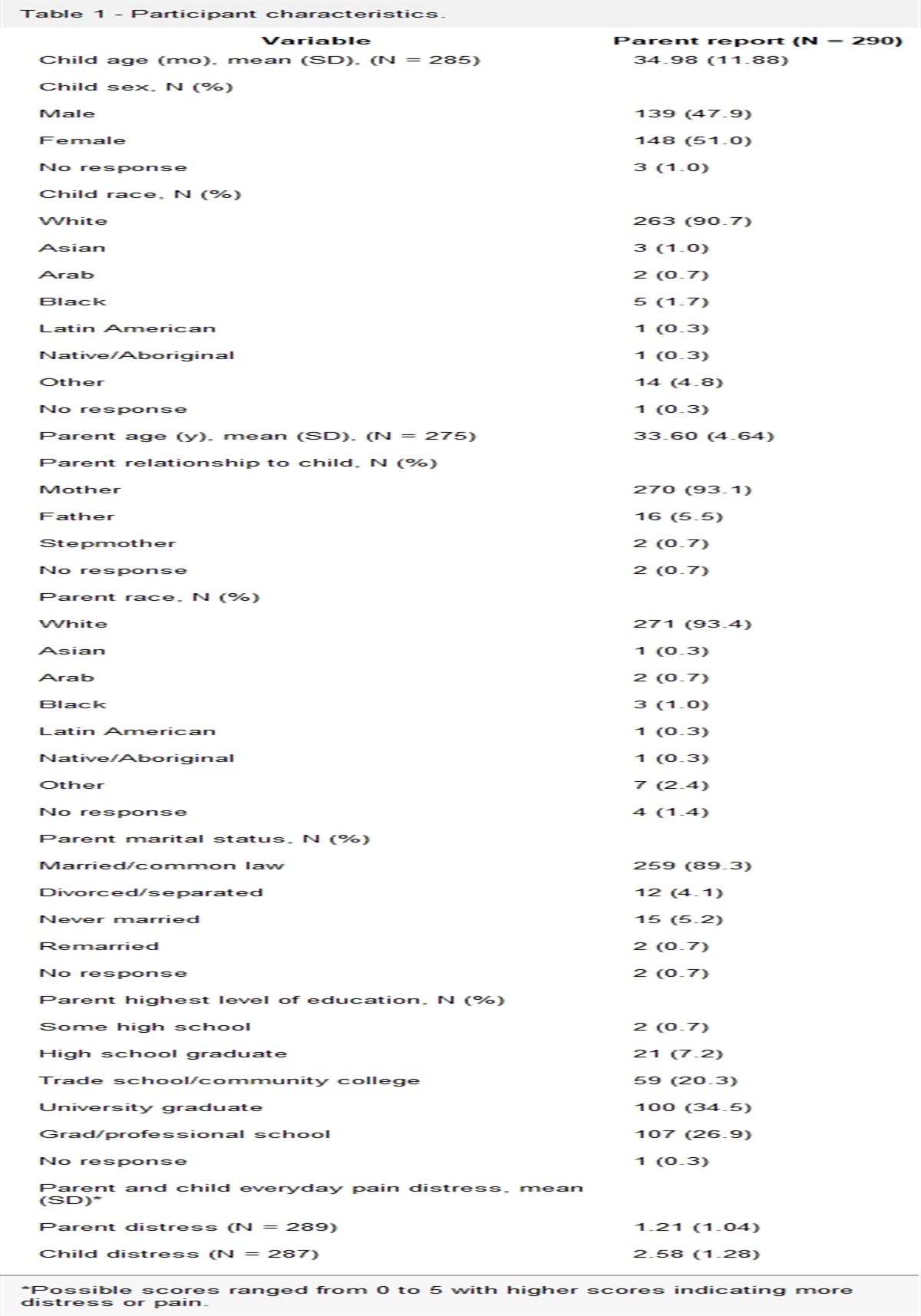
2.3. ParticipantsEight patients diagnosed with medically refractory classical TN scheduled to undergo MVD surgery at the University of Alberta Hospital were recruited and provided informed consent to participate in the study. Four additional control participants with diagnoses other than TN were also recruited: 2 undergoing MVD for hemifacial spasm (HFS) and 2 with normal pressure hydrocephalus (NPH) having in place a lumbar drain for CSF sampling. Hemifacial spasm and NPH are nonpainful conditions. A summary of participant demographics can be found in Table 1.
Table 1 - Individual participant and group characteristics. Patient ID (condition) Age in years Sex CSF collection method CSF volume collected (mL) TN 1 76 M MVD 2.5 TN 2 60 F MVD 0.6 TN 3 65 M MVD 2 TN 4 66 F MVD 3 TN 5 32 F MVD 3 TN 6 54 M MVD 3 TN 7 50 F MVD 3 TN 8 42 M MVD 3.5 TN (group) 55.6 ± 14.2 4 M; 4 F 2.6 ± 0.9 CTL 1 (HFS) 70 F MVD 2 CTL 2 (HFS) 52 M MVD 3 CTL 3 (NPH) 70 M Lumbar drain 2.5 CTL 4 (NPH) 75 F Lumbar drain 5 CTL (group) 66.8 ± 10.1 2 M; 2 F 3.1 ± 1.3Each control participant's condition is shown in parentheses in the Patient ID column. Group age and CSF volume are shown as mean ± SD.
CSF, cerebrospinal fluid; CTL, control; HFS, hemifacial spasm; MVD, microvascular decompression; NPH, normal pressure hydrocephalus; TN, trigeminal neuralgia.
During MVD, after craniotomy and durotomy are performed, the underlying arachnoid membranes are opened to gain access to the cerebellopontine angle and the TRE.15 The opening of the arachnoid membrane releases CSF (which relaxes the brain and allows for better visualization) that is normally drawn off and discarded as medical waste. In the 8 MVD patients and 2 control patients undergoing MVD for HFS, CSF samples of 0.6 to 3.5 mL were collected during this step in a sterile fashion and transported on ice from the operating room to the laboratory. Collection of cisternal CSF from the region of the trigeminal nerve is a novel approach in comparison with previous studies of CSF in patients with TN, which have collected CSF solely via lumbar puncture.1,18,46 For control patients with NPH and an implanted lumbar drain, CSF samples of 2.5 to 5 mL were collected using a sterile collection apparatus and transported on ice from the ward to the laboratory. All samples were immediately centrifuged at 1800 rpm for 5 minutes to remove any contaminant cells. Supernatant was collected as aliquots in 1.5-mL Eppendorf tubes and frozen at −80°C until analysis.
2.5. 71-plex cytokine and chemokine multiarrayMultiplex assays are an accurate and efficient way to characterize numerous proteins in a low-volume sample.47 Aliquots of each TN and control sample were sent to Eve Technologies (Calgary, AB, Canada) where the Human Cytokine/Chemokine 71-Plex Discovery Assay Array was performed. Samples were kept frozen throughout the shipping process. Designed for extracellular protein analysis in biological samples, including CSF, this multiplex assay detects 71 relevant cytokine and chemokine biomarkers found in humans: 6CKine, BCA-1, CTACK, EGF, ENA-78, Eotaxin, Eotaxin-2, Eotaxin-3, FGF-2, Flt3L, Fractalkine, G-CSF, GM-CSF, GROα, I-309, IFNα2, IFNγ, IL-1α, IL-1β, IL-1RA, IL-2, IL-3, IL-4, IL-5, IL-6, IL-7, IL-8, IL-9, IL-10, IL-12p40, IL-12p70, IL-13, IL-15, IL-16, IL-17A, IL-17E/IL-25, IL-17F, IL-18, IL-20, IL-21, IL-22, IL-23, IL-27, IL-28A, IL-33, IP-10, LIF, MCP-1, MCP-2, MCP-3, MCP-4, M-CSF, MDC, MIG, MIP-1α, MIP-1β, MIP-1δ, PDGF-AA, PDGF-AB/BB, RANTES, sCD40L, SCF, SDF-1α+β, TARC, TGFα, TNF-α, TNF-β, TPO, TRAIL, TSLP, and VEGF-A. Some samples had analyte-specific concentrations that were out of range (OOR) of the assay. For samples lesser than OOR, a value of 0 pg/mL was substituted, and for samples greater than OOR, the highest detected concentration for that analyte was substituted, as per manufacturer's instructions. Final analyte concentrations were expressed in pg/mL.
2.6. Statistical analysesTo reduce the number of comparisons required to analyze this dataset, the data were filtered for analytes that had a mean fold change >1.5 or <0.5 in the TN group compared with the control group. Fold change was calculated as: Concentration Sample/Mean Concentration Control group. In total, 19 and 21 analytes were identified as having a mean fold change >1.5 or <0.5, respectively, in the TN group. Using the ROUT method (Q = 1%),34 2 outliers were identified for the analyte RANTES in the TN group (TN 2: 241.24 pg/mL; TN 5: 1384.43 pg/mL) and 1 outlier was identified for ENA-78 in the control group (C 3: 0.870 pg/mL). These outliers were removed before analysis. Welch t tests were conducted in RStudio (Version 1.4.1106) to analyze the remaining data by looking for between-group differences in mean concentration of each biomarker. Sex differences were compared between male and female samples within the TN group. Multiple comparisons were addressed using false discovery rate (FDR) 5% correction, with significance set at q < 0.05. A cluster analysis was run to identify groupings among significantly elevated proteins in the TN group. Similarity between proteins was measured using Spearman pairwise correlation coefficients, then a bottom-up hierarchical clustering algorithm was run using the complete linkage method, which assigns each object to its own cluster then iteratively joins the 2 most similar clusters until a single cluster remains. Figures were created in RStudio and GraphPad Prism 9 (Version 9.3.0).
3. ResultsTen analytes were found to be significantly higher in the TN group compared with the control group after FDR correction: sCD40L (q = 0.033), EGF (q = 0.033), FGF-2 (q = 0.049), IL-9 (q = 0.036), IL-18 (q = 0.036), PDGF-AB/BB (q = 0.006), RANTES (q = 4.82E-6), ENA-78 (q = 0.033), IL-33 (q = 0.041), and TRAIL (q = 0.006) (all significant after FDR correction, Fig. 1). M-CSF (P = 0.033; q = 0.057) was nominally higher in the TN group but failed to survive FDR correction. Of the 21 analytes with a mean fold change <0.5 in the TN group, none were found to be significantly lower in the TN group compared with the control group. A heatmap of standardized concentrations of the 19 analytes with a mean fold change >1.5 in the TN group across study subjects is shown in Figure 2. Sample “TN 2” had uniquely elevated concentrations for several analytes, including TSLP, TPO, IL-7, IL-23, IL-17F, IL-17A, and IL-12p70 (Fig. 2). These analytes were not found to be significantly different between the 2 groups. Five main clusters were identified among the significantly elevated proteins in the TN group: ENA-78, PDGF-AB/BB, and IL-18; RANTES and TRAIL; IL-9; sCD40L and IL-33; EGF and FGF-2 (Fig. 3). There were no significant sex differences within the TN group.
 Figure 1.:
Figure 1.: Inflammatory markers significantly higher in the TN group. Concentrations (in pg/mL) of the 10 inflammatory markers found to be significantly higher in TN CSF compared with non-TN control CSF. Error bars show the SEM. Individual data points are assigned as: HFS (triangle), NPH (square), and N (circle). Significance stars are assigned as: *P < 0.05, **P < 0.01, ****P < 0.0001. CSF, cerebrospinal fluid; HFS, hemifacial spasm; PH, normal pressure hydrocephalus; TN, trigeminal neuralgia.
 Figure 2.:
Figure 2.: Heatmap of standardized concentrations for the 19 analytes with a mean fold change of >1.5 in the TN group. Each row corresponds to a specific analyte, whereas each column corresponds to a sample. C1 to C4 are from the control group and TN1 to TN8 are from the TN group. Concentrations have been standardized. TN, trigeminal neuralgia.
 Figure 3.:
Figure 3.: Clustered dendrogram and heatmap overlay of significantly elevated inflammatory markers in TN samples. Five main clusters were identified: ENA-78, PDGF-AB/BB, and IL-18 (blue); RANTES and TRAIL (purple); IL-9 (green); sCD40L and IL-33 (pink); EGF and FGF-2 (brown). The heatmap is formed from a pairwise Spearman correlation matrix. The dendrogram is labelled on the horizontal axis with its respective proteins, with a mirrored copy on the vertical axis to assist visualization of where clusters fall within the matrix. TN, trigeminal neuralgia.
4. DiscussionWe conducted an investigation of CSF from patients with TN, with specific emphasis on identifying inflammatory markers. We indeed found an altered inflammatory profile of CSF samples from patients with TN compared with non-TN control participants, identifying 10 key inflammatory markers with significantly higher concentration in the TN group.
The markers identified can be grouped based on similar function. IL-18, IL-33, and IL-9 are pro-inflammatory cytokines, with IL-18 and IL-33 both being part of the IL-1 cytokine family.10,31 IL-18 is a powerful inducer of IFNγ, another inflammatory cytokine, as well as an activator of Th1 cells and inflammatory macrophages.36 Heightened production of IL-18 correlates with disease and disease severity in several autoimmune and chronic inflammatory diseases, including MS.31 In rat models of chronic constriction injury of the sciatic nerve, microglial release of IL-18 has been linked to neuropathic pain symptoms, and blockade of this signaling attenuated pain responses.39 Similar effects have been shown in other studies, where IL-18–mediated microglia and astrocyte interactions have been established in having a key role in generating pain after nerve injury.7,32 Furthermore, complete Freund adjuvant-injection models of trigeminal neuropathic pain in mice have been linked to significant increases in IL-18 mRNA expression in trigeminal ganglion neurons.12
sCD40L and TRAIL are both part of the tumor necrosis factor (TNF) superfamily, with sCD40L being known for its pro-thrombotic and pro-inflammatory role and TRAIL being able to initiate the apoptosis pathway.3,18 Interestingly, elevated sCD40L has been linked to MS, with some MS treatments reducing serum concentrations toward normal levels.51 Ericson et al.18 found elevated TRAIL levels in TN CSF compared with controls, which then returned to similar levels as controls after MVD surgery. Our replication of increased TRAIL in a novel set of TN patients further supports its relevance in TN pathophysiology.
ENA-78 (also known as CXCL5) is a chemokine serving as chemoattractant and activator of neutrophil function that has been identified in a number of inflammatory diseases, such as ulcerative colitis48 and MS.42 Upregulation of ENA-78 has been associated with neuropathic pain in a rat model of spinal nerve injury, in which blockage of ENA-78 signaling attenuated mechanical allodynia and thermal hyperalgesia.53
EGF, PDGF-AB/BB, and FGF-2 are all growth factors that have critical developmental and homeostatic roles but are thought to contribute to various pathologies when dysregulated.2,11,52 For example, FGF-2 has been recognized as a potential contributor to the pathogenesis of inflammatory diseases such as MS and rheumatoid arthritis.52 However, growth factors may be released from damaged neurons as a neuroprotective mechanism, as has been shown by PDGF-BB protecting dopaminergic neurons in animal models of Parkinson disease and FGF-2 exerting microglia-induced neuroprotection.13,35 Furthermore, overexpression of FGF-2 has been shown to attenuate epileptogenesis-associated neuroinflammation in rats, especially by reducing IL-1β expression.9 Elevation of these growth factors may represent a response to demyelination because these factors are involved in oligodendrocyte progenitor propagation.37 To date, our study is the first to report elevations in these growth factors in TN CSF, and identifying their exact role in TN pathogenesis is a key future direction.
RANTES, a proinflammatory chemokine otherwise known as CCL5, was very high in TN CSF and almost nonexistent in control CSF, which makes it an interesting candidate for further study. In inflammatory conditions, RANTES is upregulated and attracts T cells, causing them to proliferate and activate.54 T helper 1 cells release IFNγ subsequently increasing RANTES expression, leading to a cycle that further prolongs the inflammatory response.54 Furthermore, RANTES has been linked to atypical facial pain (AFP) and trigeminal-mediated pain previously.27 A study of medullary jawbone samples from 15 patients with fatty-degenerative osteolysis and osteonecrosis of the jawbone with concomitant AFP or TN found a 30-fold overexpression of RANTES compared with healthy jawbones.27 A proposed mechanism of action by RANTES in pain is the desensitization of mu opioid receptors in peripheral sensory neurons, therefore modifying the nociceptive reaction.27 It can also attract dendritic cells, eosinophils, natural killer cells, mast cells, and basophils to sites of inflammation and infection.28 Notably, CSF RANTES levels in healthy individuals are very low but increase dramatically at the onset and progression of MS.33,40 Furthermore, RANTES can increase synaptic excitability by enhancing glutamatergic transmission in vitro.33 Taken together, these previous findings in conjunction with our confirmation of significant RANTES elevation implicates RANTES as a key player in the inflammatory nature of TN.
Overall, the key inflammatory mediators identified in this study have a widespread role in inflammatory processes and have been implicated in other disease states, especially MS. In the context of neuropathic pain, neuroinflammation can impact 4 main processes. First, it leads to increased vascular permeability, leukocyte infiltration, glial cell activation, and increased production of inflammatory mediators (cytokines and chemokines).25 Second, inflammatory mediators can directly activate and sensitize nociceptors, which leads to pain.26,30 Third, neuroinflammation is also known to increase the expression of ion channels involved in peripheral sensitization, such as transient receptor potential ion channels and sodium channels.30 Finally, immune cells and neurons communicate via inflammatory mediators, which modulates the response to injury through regulating resident immune cells and recruiting immune cells to the injured area.30 We speculate that these mechanisms may lead to peripheral sensitization and foster the development or maintenance of TN. Notably, the IL-1 and TNF families of ligands have been recognized as key players in the sensitizing mechanisms of neuropathic pain.14
Trigeminal neuralgia is more common in females than males, presenting in an approximately 1.5 to 2:1 ratio.6,16 However, we did not find any differences between female TN CSF and male TN CSF in our sample. It is possible that our sample was not sufficiently large enough to detect sex differences. Future research should continue to investigate sex differences in TN CSF because of its clinical relevance.
The cluster analysis yielded 5 main groupings of the inflammatory proteins that were significantly elevated in the TN group. Interestingly, these clusters do not group the proteins within the “protein families” (cytokines, chemokines, TNF superfamily, and growth factors) that our discussion is largely based around. However, it may suggest that multiple co-regulated molecular pathways involved in the inflammatory pathogenesis of TN exist and contain members of different protein families. For example, the cluster of ENA-78 (chemokine), PDGF-AB/BB (growth factor), and IL-18 (interleukin) may represent a co-regulated inflammatory pathway that contributes to the overall inflammation in patients with TN. Further research should aim to elucidate the true relationships between inflammatory proteins involved in the pathogenesis of TN.
This study is limited by a relatively small sample size and a control group that contains 2 distinct—though nonpainful—conditions (ie, HFS and NPH) with CSF extracted from 2 different sites (ie, cisternal and lumbar), only one of which matched the cisternal site of TN CSF acquisition. We intentionally chose to collect cisternal CSF from around the trigeminal nerve in patients undergoing MVD, based on the rationale that this might enhance the sensitivity of our TN CSF samples to the inflammatory environment experienced by trigeminal neurons compared with previous studies that solely used lumbar puncture CSF samples distant from the site of TN pathology.1,18,46 Ethical challenges obviously prevented us from extracting cisternal CSF from completely healthy populations. Although it is true that cisternal CSF may be encountered in a variety of neurosurgical procedures, the vast majority of these are for tumor-related surgery, in which a confounding pro-inflammatory local environment is highly likely to be present; consequently, we limited cisternal control CSF collection to HFS patients. There is no doubt that lumbar CSF from NPH patients represents an imperfect control for comparison with cisternal TN CSF. That being said, previous work in NPH patients has shown an increasing gradient of complement factors from cisternal to lumbar CSF,44 meaning that our use of lumbar NPH CSF is unlikely to have exaggerated the pro-inflammatory profile of TN CSF that we identified. A limitation to the generalization of study findings stems from the exclusive use of classical TN patients with evidence of NVC. With DTI studies finding evidence of microstructural abnormalities in idiopathic TN despite the absence of NVC, inflammatory processes may also be at play to cause damage. The current study does not address the role of neuroinflammation in idiopathic TN because of evidence of NVC being a common inclusion criterion for MVD surgery. Ultimately, despite these limitations, we were able to detect strong and statistically significant differences between patients with TN and non-TN control participants after correction for multiple comparisons, suggesting that these differences were truly driven by the presence of increased inflammation in TN.
5. ConclusionPatients with TN have increased inflammatory markers in the CSF compared with pain-free control participants. This includes pro-inflammatory cytokines, TNF superfamily, chemokines, and growth factors that may all play distinct, contributory roles to TN pathophysiology. Overall, this study contributes to the growing body of literature demonstrating that inflammation is present in TN.
DisclosuresThe authors have no conflict of interest to declare.
AcknowledgmentsThis work was supported by the Edmonton Civic Employees Charitable Assistance Fund (B.J.K. and T.S.); a Project Grant from the Canadian Institutes of Health Research (CIHR) (B.J.K.). FRN:162434; and the Alexander Graham Bell Canada Graduate Scholarship—Doctoral Program (CGS-D) from the Natural Sciences and Engineering Research Council of Canada (NSERC) (TNF).
Data availability statement: The data that support the findings of this study are available from the corresponding author, T.S., upon reasonable request.
References [1]. Abu Hamdeh S, Khoonsari PE, Shevchenko G, Gordh T, Ericson H, Kultima K. Increased CSF levels of apolipoproteins and complement factors in trigeminal neuralgia patients-in depth proteomic analysis using mass spectrometry. J Pain 2020;21:1075–84. [2]. Andrae J, Gallini R, Betsholtz C. Role of platelet-derived growth factors in physiology and medicine. Genes Dev 2008;22:1276–312. [3]. Antoniades C, Bakogiannis C, Tousoulis D, Antonopoulos AS, Stefanadis C. The CD40/CD40 ligand system: linking inflammation with atherothrombosis. J Am Coll Cardiol 2009;54:669–77. [4]. Antonini G, Di Pasquale A, Cruccu G, Truini A, Morino S, Saltelli G, Romano A, Trasimeni G, Vanacore N, Bozzao A. Magnetic resonance imaging contribution for diagnosing symptomatic neurovascular contact in classical trigeminal neuralgia: a blinded case-control study and meta-analysis. PAIN 2014;155:1464–71. [5]. Bach FW, Langemark M, Ekman R, Rehfeld JF, Schifter S, Olesen J. Effect of sulpiride or paroxetine on cerebrospinal fluid neuropeptide concentrations in patients with chronic tension-type headache. Neuropeptides 1994;27:129–36. [6]. Bendtsen L, Zakrzewska JM, Heinskou TB, Hodaie M, Leal PRL, Nurmikko T, Obermann M, Cruccu G, Maarbjerg S. Advances in diagnosis, classification, pathophysiology, and management of trigeminal neuralgia. Lancet Neurol 2020;19:784–96. [7]. Bian C, Wang ZC, Yang JL, Lu N, Zhao ZQ, Zhang YQ. Up-regulation of interleukin-23 induces persistent allodynia via CX3CL1 and interleukin-18 signaling in the rat spinal cord after tetanic sciatic stimulation. Brain Behav Immun 2014;37:220–30. [8]. Bick SKB, Eskandar EN. Surgical treatment of trigeminal neuralgia. Neurosurg Clin N Am 2017;28:429–38. [9]. Bovolenta R, Zucchini S, Paradiso B, Rodi D, Merigo F, Navarro Mora G, Osculati F, Berto E, Marconi P, Marzola A, Fabene PF, Simonato M. Hippocampal FGF-2 and BDNF overexpression attenuates epileptogenesis-associated neuroinflammation and reduces spontaneous recurrent seizures. J Neuroinflammation 2010;7:81. [10]. Chakraborty S, Kubatzky KF, Mitra DK. An update on interleukin-9: from its cellular source and signal transduction to its role in immunopathogenesis. Int J Mol Sci 2019;20:2113. [11]. Chen J, Zeng F, Forrester SJ, Eguchi S, Zhang MZ, Harris RC. Expression and function of the epidermal growth factor receptor in physiology and disease. Physiol Rev 2016;96:1025–69. [12]. Chen ML, Lin K, Lin SK. NLRP3 inflammasome signaling as an early molecular response is negatively controlled by miR-186 in CFA-induced prosopalgia mice. Braz J Med Biol Res 2018;51:e7602. [13]. Chen H, Teng Y, Chen X, Liu Z, Geng F, Liu Y, Jiang H, Wang Z, Yang L. Platelet-derived growth factor (PDGF)-BB protects dopaminergic neurons via activation of Akt/ERK/CREB pathways to upregulate tyrosine hydroxylase. CNS Neurosci Ther 2021;27:1300–12. [14]. Clark AK, Old EA, Malcangio M. Neuropathic pain and cytokines: current perspectives. J Pain Res 2013;6:803–14. [15]. Cohen-Gadol AA. Microvascular decompression surgery for trigeminal neuralgia and hemifacial spasm: naunces of the technique based on experiences with 100 patients and review of the literature. Clin Neurol Neurosurg 2011;113:844–53. [16]. De Toledo IP, Conti Reus J, Fernandes M, Porporatti AL, Peres MA, Takaschima A, Linhares MN, Guerra E, De Luca Canto G. Prevalence of trigeminal neuralgia: a systematic review. J Am Dent Assoc 2016;147:570–76 e572. [17]. DeSouza DD, Hodaie M, Davis KD. Abnormal trigeminal nerve microstructure and brain white matter in idiopathic trigeminal neuralgia. PAIN 2014;155:37–44. [18]. Ericson H, Abu Hamdeh S, Freyhult E, Stiger F, Bäckryd E, Svenningsson A, Gordh T, Kultima K. Cerebrospinal fluid biomarkers of inflammation in trigeminal neuralgia patients operated with microvascular decompression. PAIN 2019;160:2603–11. [19]. Fujiwara S, Sasaki M, Wada T, Kudo K, Hirooka R, Ishigaki D, Nishikawa Y, Ono A, Yamaguchi M, Ogasawara K. High-resolution diffusion tensor imaging for the detection of diffusion abnormalities in the trigeminal nerves of patients with trigeminal neuralgia caused by neurovascular compression. J Neuroimaging 2011;21:e102–8. [20]. Hamlyn PJ, King TT. Neurovascular compression in trigeminal neuralgia: a clinical and anatomical study. J Neurosurg 1992;76:948–54. [21]. Harrington MG. Cerebrospinal fluid biomarkers in primary headache disorders. Headache 2006;46:1075–87. [22]. Headache Classification Committee of the International Headache Society (IHS). The international classification of headache disorders, 3rd edition. Cephalalgia 2018;38:1–211. [23]. Herweh C, Kress B, Rasche D, Tronnier V, Tröger J, Sartor K, Stippich C. Loss of anisotropy in trigeminal neuralgia revealed by diffusion tensor imaging. Neurology 2007;68:776–8. [24]. Hilton DA, Love S, Gradidge T, Coakham HB. Pathological findings associated with trigeminal neuralgia caused by vascular compression. Neurosurgery 1994;35:299–303; discussion 303. [25]. Ji RR, Xu ZZ, Gao YJ. Emerging targets in neuroinflammation-driven chronic pain. Nat Rev Drug Discov 2014;13:533–48. [26]. Ji RR, Nackley A, Huh Y, Terrando N, Maixner W. Neuroinflammation and central sensitization in chronic and widespread pain. Anesthesiology 2018;129:343–66. [27]. Lechner J, von Baehr V. Peripheral neuropathic facial/trigeminal pain and RANTES/CCL5 in jawbone cavitation. Evid Based Complement Alternat Med 2015;2015:582520. [28]. Levy JA. The unexpected pleiotropic activities of RANTES. J Immunol 2009;182:3945–6. [29]. Maarbjerg S, Wolfram F, Gozalov A, Olesen J, Bendtsen L. Significance of neurovascular contact in classical trigeminal neuralgia. Brain 2015;138:311–9. [30]. Matsuda M, Huh Y, Ji RR. Roles of inflammation, neurogenic inflammation, and neuroinflammation in pain. J Anesth 2019;33:131–9. [31]. Migliorini P, Italiani P, Pratesi F, Puxeddu I, Boraschi D. The IL-1 family cytokines and receptors in autoimmune diseases. Autoimmun Rev 2020;19:102617. [32]. Miyoshi K, Obata K, Kondo T, Okamura H, Noguchi K. Interleukin-18-mediated microglia/astrocyte interaction in the spinal cord enhances neuropathic pain processing after nerve injury. J Neurosci 2008;28:12775–87. [33]. Mori F, Nisticò R, Nicoletti CG, Zagaglia S, Mandolesi G, Piccinin S, Martino G, Finardi A, Rossini PM, Marfia GA, Furlan R, Centonze D. RANTES correlates with inflammatory activity and synaptic excitability in multiple sclerosis. Mult Scler 2016;22:1405–12. [34]. Motulsky HJ, Brown RE. Detecting outliers when fitting data with nonlinear regression—a new method based on robust nonlinear regression and the false discovery rate. BMC Bioinformatics 2006;7:123. [35]. Noda M, Takii K, Parajuli B, Kawanokuchi J, Sonobe Y, Takeuchi H, Mizuno T, Suzumura A. FGF-2 released from degenerating neurons exerts microglial-induced neuroprotection via FGFR3-ERK signaling pathway. J Neuroinflammation 2014;11:76. [36]. Novick D, Kim S, Kaplanski G, Dinarello CA. Interleukin-18, more than a Th1 cytokine. Semin Immunol 2013;25:439–48. [37]. Oliveira SL, Pillat MM, Cheffer A, Lameu C, Schwindt TT, Ulrich H. Functions of neurotrophins and growth factors in neurogenesis and brain repair. Cytometry A 2013;83:76–89. [38]. Peker S, Kurtkaya O, Uzün I, Pamir MN. Microanatomy of the central myelin-peripheral myelin transition zone of the trigeminal nerve. Neurosurgery 2006;59:354–59; discussion 354-9. [39]. Pilat D, Piotrowska A, Rojewska E, Jurga A, Slusarczyk J, Makuch W, Basta-Kaim A, Przewlocka B, Mika J. Blockade of IL-18 signaling diminished neuropathic pain and enhanced the efficacy of morphine and buprenorphine. Mol Cell Neurosci 2016;71:114–24. [40]. Pittaluga A. CCL5-Glutamate cross-talk in astrocyte-neuron communication in multiple sclerosis. Front Immunol 2017;8:1079. [41]. Rappaport ZH, Govrin-Lippmann R, Devor M. An electron-microscopic analysis of biopsy samples of the trigeminal root taken during microvascular decompressive surgery. Stereotact Funct Neurosurg 1997;68:182–6. [42]. Rumble JM, Huber AK, Krishnamoorthy G, Srinivasan A, Giles DA, Zhang X, Wang L, Segal BM. Neutrophil-related factors as biomarkers in EAE and MS. J Exp Med 2015;212:23–35. [43]. Sakka L, Coll G, Chazal J. Anatomy and physiology of cerebrospinal fluid. Eur Ann Otorhinolaryngol Head Neck Dis 2011;128:309–16. [44]. Seele J, Kirschfink M, Djukic M, Lange P, Gossner J, Bunkowski S, Wiltfang J, Nau R. Cisterno-lumbar gradient of complement fractions in geriatric patients with suspected normal pressure hydrocephalus. Clin Chim Acta 2018;486:1–7. [45]. Strittmatter M, Grauer M, Isenberg E, Hamann G, Fischer C, Hoffmann KH, Blaes F, Schimrigk K. Cerebrospinal fluid neuropeptides and monoaminergic transmitters in patients with trigeminal neuralgia. Headache 1997;37:211–6. [46]. Svedung Wettervik T, Folkvaljon D, Gordh T, Freyhult E, Kultima K, Ericson H, Abu Hamdeh S. Cerebrospinal fluid in classical trigeminal neuralgia: an exploratory study on candidate biomarkers. Biomedicines 2022;10:998. [47]. Tighe PJ, Ryder RR, Todd I, Fairclough LC. ELISA in the multiplex era: potentials and pitfalls. Proteomics Clin Appl 2015;9:406–22. [48]. Walz A, Schmutz P, Mueller C, Schnyder-Candrian S. Regulation and function of the CXC chemokine ENA-78 in monocytes and its role in disease. J Leukoc Biol 1997;62:604–11. [49]. Wesenhagen KEJ, Teunissen CE, Visser PJ, Tijms BM. Cerebrospinal fluid proteomics and biological heterogeneity in Alzheimer's disease: a literature review. Crit Rev Clin Lab Sci 2020;57:86–98. [50]. Wu M, Qiu J, Jiang X, Li M, Wang SD, Dong Q, Fu X, Niu C. Diffusion tensor imaging reveals microstructural alteration of the trigeminal nerve root in classical trigeminal neuralgia without neurovascular compression and correlation with outcome after internal neurolysis. Magn Reson Imaging 2020;71:37–44. [51]. Wu Q, Wang Q, Yang J, Martens JW, Mills EA, Saad A, Chilukuri P, Dowling CA, Mao-Draayer Y. Elevated sCD40L in secondary progressive multiple sclerosis in comparison to non-progressive benign and relapsing remitting multiple sclerosis. J Cent Nerv Syst Dis 2021;13:11795735211050712. [52]. Xie Y, Su N, Yang J, Tan Q, Huang S, Jin M, Ni Z, Zhang B, Zhang D, Luo F, Chen H, Sun X, Feng JQ, Qi H, Chen L. FGF/FGFR signaling in health and disease. Signal Transduct Target Ther 2020;5:181. [53]. Xu W, Zhu M, Yuan S, Yu W. Spinal CXCL5 contributes to nerve injury-induced neuropathic pain via modulating GSK-3β phosphorylation and activity in rats. Neurosci Lett 2016;634:52–9. [54]. Zeng Z, Lan T, Wei Y, Wei X. CCL5/CCR5 axis in human diseases and related treatments. Genes Dis 2022;9:12–27.
留言 (0)