Study participants
This was a retrospective big data study of children < 18 years old without any underlying diseases, that visited the ED with symptoms of acute diarrhea during a 34-month period from 2018 to 2022, at a tertiary care, academic medical center in Seoul, South Korea. The first 17 months of the study period (From April 1, 2018 to September 30, 2019) was the period before the rapid syndromic multiplex GI pathogen panel (GI panel) was incorporated, the pre-implementation period, and the latter 17 months of the study period (From April 1, 2021 to August 31, 2022) was the post-implementation period. Between the pre-implementation period and the post-implementation period, there was an introduction period in which the GI panel test system was introduced to allow the medical staff to adapt. The GI panel that was incorporation in the ED was the BioFire ® FilmArray ® GI Panel (BioFire diagnostics, Salt Lake City, United States), which is able to detect the following 22 pathogens: Campylobacter (C. jejuni/C. coli /C. upsaliensis), Clostridioides (Clostridium) difficile (toxin A/B), Plesiomonas shigelloides, Salmonella, Yersinia enterocolitica, Vibrio (V. parahaemolyticus/V. vulnificus/V. cholerae), Enteroaggregative E. coli (EAEC), Enteropathogenic E. coli (EPEC), Enterotoxigenic E. coli (ETEC) lt/st, Shiga-like toxin-producing E. coli (STEC) stx1/stx2, E. coli O157, Shigella/Enteroinvasive E. coli (EIEC), Cryptosporidium, Cyclospora cayetanensis, Entamoeba histolytica, Giardia lamblia, Adenovirus F40/41, Astrovirus, Norovirus GI/GII, Rotavirus A, and Sapovirus (I, II, IV, and V).
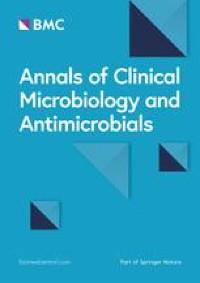
The inclusion criteria were as follows: Patients that were 1) below 18 years of age, 2) visited the ED for acute diarrhea, 3) acute symptoms that began within 72 h, and had moderate to severe diarrhea, with moderate defined as 6–9 stools/day and severe defined as > 10 stools/day [20]. The exclusion criteria were as follows: 1) immunocompromised patients, 2) patients with chronic underlying medical conditions, 3) patients with inflammatory bowel disease or other chronic gastrointestinal disorders, and 4) considered mild acute infectious diarrhea, defined as mean stool frequency of 5 or less stools/day and mild degree of dehydration were excluded. Patients with mild acute infectious diarrhea were excluded from the study because majority were discharged from the ED without blood or stool tests.
Study design
This was a big data analytical study using Seoul St. Mary’s hospital’s healthcare data warehouse which encompasses each patient’s clinical information, laboratory and image results, vital signs, and administrative information (ie. ED arrival, ED discharge time, ward transfer time, laboratory specimen submission times, laboratory results reporting times, etc.). Patients that fit the inclusion criteria were included as study participants and the following demographic and clinical parameters were extracted from the hospital’s corporate data warehouse: date of visit, age at visit, sex, ED arrival time and date, ED discharge time and date, any revisits within 7 days after ED discharge, time and date of ward transfer from the ED, discharge date from ward, date of outpatient clinic follow up after ED, admission from outpatient clinic after ED discharge, time and date of isolation, all types of antibiotics administered, GI panel results, laboratory findings, image findings (including abdominal x-rays, CT, ultrasound), blood culture and stool culture results, and date of pediatric intensive care unit transfer. All patient data was de-identified of all identifiers after retrieval.
After the GI panel was implemented in the ED, it was prescribed to patients with symptoms of acute diarrhea of moderate to severe symptoms, with clinically suspicious infectious etiology. Whether to prescribe the GI panel to the patient or not was the decision of the clinician treating the patient in the ED, however, was mainly decided considering the following: 1) need for hospitalization, 2) severity of symptoms, 3) subjective decision as to whether the patient will benefit from the test results, and 4) agreement of the guardians. The unformed stool specimens were collected by Copan flocked swab (FLOQSwab™, Copan, Murrieta, United States) and transported in 2 mL of Cary-Blair medium which was then immediately submitted to the hospital’s laboratory. The results were provided within 2–3 h of stool submission.
Ethics approval made by Seoul St. Mary’s hospital’s Data Review Board and Institutional Review Board (IRB no. KC22RISI0669) in accordance with the Declaration of Helsinki. This study was retrospective in design and data used for this study did not include any identifiers and thus informed consent was waived by the review board.
Outcome measures and definitions
The primary outcome was assessing the following four clinical decision parameters. First, the clinician’s decision to prescribe antibiotics was assessed by observing changes in the proportion of patients prescribed broad spectrum antibiotics pre- and post-implementation of the GI panel, regardless of the pathogen identified. Second, knowing the etiologic pathogen of acute diarrhea can possibly reduce the number of additional imaging modalities such as abdominal ultrasounds or abdominal computer tomography (CT) prescribed in the ED. Therefore, the physician’s decision to undergo additional imaging modalities in the ED to rule out other focuses such as surgical abdomen or hidden infections was assessed by observing changes in the number of ultrasounds and CTs. Third, changes in infection prevention and control measures was analyzed by observing changes in 1) the number of consults made to infectious disease specialist for appropriate transmission prevention interventions, and 2) time to achieving appropriate isolation measures in patients.
The secondary outcome was assessing the following patient outcome parameters pre- and post-implementation of the GI panel: 1) changes in the duration of ED stay, 2) the number of ED revisit within 7 days for the same episode of acute diarrhea, 3) hospitalization rate from the outpatient clinic after discharge from the ED, and 4) changes in disease progression rate or patients that eventually were treated in the intensive care unit.
Definitions
The outcome measures were compared between the two periods, pre- and post-implementation of the GI panel. The length of ED stay was determined by ED discharge time minus ED arrival time. The hospitalization rate was defined as the number of patients admitted from the ED divided by the number of total patients that visited the ED. The length of hospitalization was defined as the time and date of discharge from the ward minus the time and date of ward transfer from the ED. The percentage of antibiotic usage was determined as the percentage of patients that were prescribed any type of antibiotics (intravenous or oral) for acute diarrhea. Appropriate isolation measure was defined as patients that were intervened with the appropriate transmission prevention isolation measure depending on the identified pathogen. Time to appropriate isolation measures was defined as the time and date of execution of appropriate isolation measure minus the time and date of admission from the ED. Broad spectrum antibiotics was defined as antibiotics that kills or inhibits both gram positive and gram negative bacteria or a wide range of bacteria that causes diseases [21].
Statistical analyses
P-values were calculated using chi-square test for categorical variables and t-test or wilcoxon rank sum test for continuous variables. Linear regression analyses were used to observe trends in outcomes after the implementation of the syndromic GI panel test in the ED. Interrupted time series regression analysis was used to observe the statistical significance of the immediate effects of incorporating the GI panel in the ED. In this study, the interrupted time series (ITS) model estimated the immediate change associated with the time point (change in level) and the change in slope from the baseline trend to the post-time point direction (change in trend). We used the Durbin-Watson test to detect autocorrelation. At the same time, we used SAS Proc AUTOREG with the BACKSTEP option to automatically select the correct order of the autoregressive model through backward elimination from an initial full model with order (k) = 12. Model fit was assessed using visual plots (autocorrelation function, partial autocorrelation function white noise probabilities, and autocorrelation functions). All analyses were conducted using SAS version 9.4 (SAS Institute, Cary, NC, USA) and R software version 4.1.2 (R Foundation for Statistical Computing, Vienna, Austria). All tests were two sided, and a P value < 0.05 was regarded as statistically significant.




留言 (0)