
記住我

Hernia, also known as “hernia,” is a phenomenon in which a part of an individual’s internal organs or tissues leaves its original position and enters another part of the body through congenital or acquired gaps, defects, or weak areas.[1] Currently, hernia can be distinguished as abdominal hernia, lumbar hernia, brain hernia, etc. based on the location of hernia, and hernia appearing in the abdomen is known as abdominal hernia, which can be subdivided into abdominal external hernia and abdominal internal hernia.[2] Inguinal hernia is a common type of abdominal external hernia, accounting for more than 90% of the external abdominal hernia, with nearly 90% of the patients being male and only about 10% being female; the age group where inguinal hernia is prevalent is bimodal, with the highest prevalence in the age group of 0–5 and 75–80 years.[3]
Typical inguinal hernia includes hernia content, hernia sac, hernia ring, and hernia outer tegmentum. Clinical treatment of patients with inguinal hernia should be carried out according to the specific conditions of the patients. At present, according to the occurrence site of inguinal hernia, it can be subdivided into indirect hernia, direct hernia, femoral hernia, compound hernia, and perifemoral hernia, and according to the contents of the hernia, it can be divided into recurrent hernia, refractory hernia, incarcerated hernia, strangulated hernia.[4] The diagnosis of inguinal hernia mainly depends on the medical history, clinical manifestations of the patients and physical examination. Generally, most inguinal hernias can be clearly diagnosed through medical history and physical examination. If the cause of the patient is unknown, or there is swelling and pain in the local area, ultrasound detection can also be supplemented to improve the diagnostic accuracy.[5]
Early surgical treatment is recommended for patients with inguinal hernia with clinical symptoms. Taking incarcerated hernia in inguinal hernia as an example, such patients often present with painful manifestations and are at risk of developing intestinal obstruction if left untreated.[6] Minimally invasive surgery represented by laparoscopy is more widely used in the treatment of inguinal hernia, and compared with traditional open hernia repair, laparoscopic inguinal hernia repair (LIHR) has the advantages of less trauma, less pain, and rapid postoperative recovery of the patient.[7] However, even if laparoscopic surgery effectively reduces the trauma to patients, patients with inguinal hernia undergoing laparoscopic surgery will still experience postoperative complications such as chronic pain and temporary skin paresthesia, which will reduce the patient’s evaluation of the surgery, and even induce the emergence of patient-doctor conflicts. If specific interventions can be implemented for the risk factors of postoperative complications in patients with LIHR, it will help to improve the surgical experience of the patients, shorten the length of the postoperative hospital stay, and increase the efficiency of the use of healthcare resources, which is also an innovative aspect of the present study.[8,9] Through a retrospective analysis, this study found that body mass index (BMI), intraoperative blood loss, medical history time, intraoperative adhesions, abnormal coagulation function, recurrent hernia, and hypertension were the risk factors for complications after LIHR. Details are described as follows.
2. Materials and methods 2.1. Design methods and patientsThis study was conducted by retrospective analysis and was approved by the ethics committee of Yongjia County Traditional Chinese Medicine Hospital. Clinical data of patients undergoing LIHR in our hospital from July 2020 to October 2022 were collected by accessing electronic medical records. The inclusion criteria were set as follows: all patients had a definite diagnosis of inguinal hernia before surgery (with Guidelines for Diagnosis and Treatment of Inguinal Hernia in Adults[10] as the reference standard) and received laparoscopic surgical treatment in our hospital; patients aged ≥ 18 years; patients with complete clinical data (age, sex, BMI, hernia classification, hernia sac management, surgical method, etc.); and patients with complete postoperative follow-up data (with or without complications). The exclusion criteria were set as follows: patients complicated with severe liver and kidney dysfunctions; patients with missing preoperative laboratory indicators; patients who converted to laparotomy during laparoscopic surgery; patients complicated with malignant tumor; patients complicated with tissue healing disorder; patients with long-term use of glucocorticoids; patients with incomplete postoperative follow-up data; and patients with concurrent mental dysfunction.
2.2. Data collectionThe following data were collected from the electronic medical records: baseline clinical information (age, sex, BMI), hernia classification (indirect hernia, direct hernia, compound hernia, femoral hernia), hernia sac management (complete dissection, hernia sac transection), surgical approach [transabdominal preperitoneal (TAPP), total extraperitoneal (TEP)], type of patch (lightweight, heavyweight), operative time, intraoperative blood loss, diabetes mellitus (yes/no), hypertension (yes/no), intraoperative adhesions (yes/no), abnormal coagulation function (yes/no), and recurrent hernia (yes/no).
Postoperative complications included seroma, hematoma, surgical site infection, chronic pain, skin paresthesia, urinary retention, paralytic intestinal obstruction, etc.
Data collection was done by investigators and patient-responsible physicians, and data collection began in July 2020 and ended in October 2022. Patients were followed up until May 2023.
2.3. Outcome measurement and statistical analysisAfter data collection and screening, a total of 212 patients who received LIHR in our hospital from July 2020 to October 2022 met the inclusion and exclusion criteria, including 36 patients with complications and 176 patients without complications.
The data collected from the patients was processed using Statistical Package for the Social Sciences 22.0. The measurement data were expressed in the form of (mean ± standard deviation) using the t test, while the count data were expressed in the form of rate using the chi-square test. The data with statistical significance in the chi-square test were included in the multivariate Logistic regression analysis model to continue the validation of the difference, and the difference was considered to be statistically significant at P < .05.
3. Results 3.1. General data of perioperative periodA total of 212 patients undergoing LIHR were included in this study. Among them, there were 13 cases of femoral hernia, 97 cases of indirect hernia, 92 cases of direct hernia, and 10 cases of indirect hernia + direct hernia. The distribution of disease types is shown in Figure 1. There were 53 cases treated with TAPP and 159 cases with TEP. The mean operative time was (76.26 ± 12.56) minutes. The average length of hospital stay was (3.29 ± 1.53) days.
 Figure 1.:
Figure 1.: Distribution of disease types in patients undergoing laparoscopic inguinal hernia repair.
3.2. Presentation of the follow-up of enrolled patientsThe enrolled patients were followed up for 12 to 34 months, with a median follow-up of 26 months. Among the 212 patients successfully followed up, 36 patients had complications. Among the patients with complications, there were 10 cases of seroma and hematoma, 9 cases of postoperative urinary retention, 9 cases of postoperative unexplained chronic pain, 4 cases of foreign body sensation and groin skin paresthesia, 1 case of surgical site infection, 1 case of subcutaneous abscess, 1 case of patch infection, and 1 case of paralytic intestinal obstruction (Fig. 2).
 Figure 2.:
Figure 2.: Analysis of complications in patients undergoing laparoscopic inguinal hernia repair.
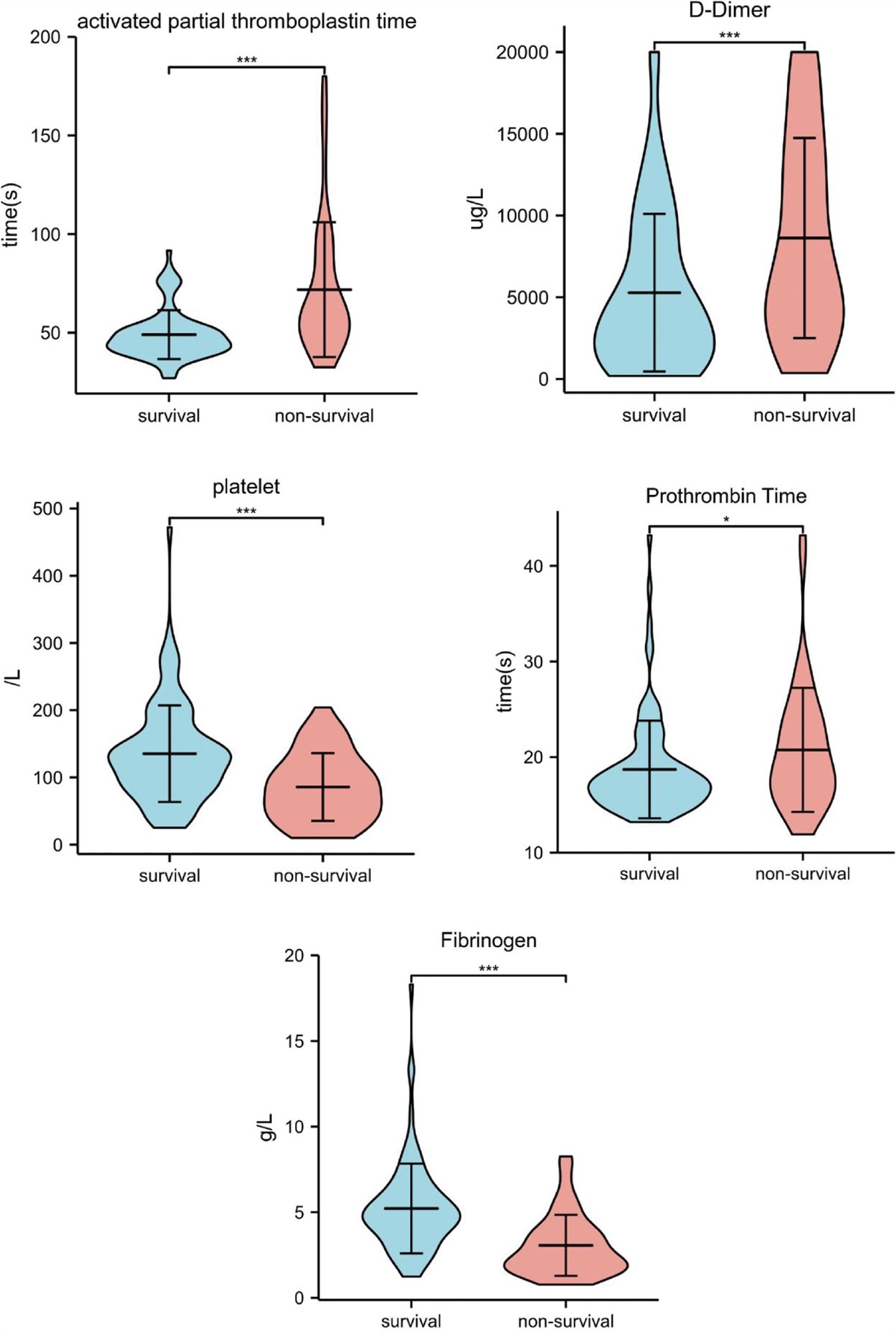
3.3. Univariate analysis of risk factors for postoperative complicationsPatients were divided into complication group (n = 36) and non-complication group (n = 176) according to whether they had complications after surgery. Clinical data (age, sex, BMI), hernia classification (indirect hernia, direct hernia, compound hernia, femoral hernia), hernia sac management (complete dissection, hernia sac transection), surgical approach (TAPP, TEP), type of patch (lightweight, heavyweight), operative time, intraoperative blood loss, diabetes mellitus (yes/no), hypertension (yes/no), intraoperative adhesions (yes/no), abnormal coagulation function (yes and no), and recurrent hernia (yes/no) were collected in detail through the in-hospital information system. Then, the differences of above data collected from the 2 groups were compared. The results showed that there were statistically significant differences in BMI, intraoperative blood loss, hernia sac management, intraoperative adhesions, abnormal coagulation function, recurrent hernia, and hypertension between the 2 groups (P < .05), as shown in Table 1 and Figure 3.
Table 1 - Clinical data and complications of patients undergoing laparoscopic inguinal hernia repair. General clinical data Complication group (n = 36) Non-complication group (n = 176) t/χ2 P Case Rate (%) Case Rate (%) Sex Male 26 72.22 123 69.89 2.107 .147 Female 10 27.78 53 30.11 Mean age (yr) 44.58 ± 10.33 45.36 ± 9.71 0.060 .952 BMI (kg/m2) 26.30 ± 2.91 22.89 ± 2.92 6.809 <.001 Blood glucose (mmol/L) 5.57 ± 1.24 5.40 ± 0.94 0.068 .946 Hemoglobin (g/L) 147.90 ± 10.27 148.91 ± 9.82 0.175 .861 Operative time (min) 77.23 ± 10.63 77.22 ± 10.51 0.243 .808 Intraoperative blood loss (mL) 8.69 ± 1.14 7.05 ± 1.08 13.393 <.001 Medical history time (months) 47.68 ± 28.92 33.11 ± 18.68 5.371 <.001 Hernia classification Indirect hernia 20 55.56 63 35.80 0.551 .631 Direct hernia 14 38.89 93 52.84 Compound hernia 1 2.78 11 6.25 Femoral hernia 1 2.78 9 5.11 Hernia sac management Complete dissection 21 58.33 96 54.55 5.775 .016 Hernia sac transection 15 41.67 80 45.45 Intraoperative adhesions Yes 16 44.44 26 14.77 4.128 .042 No 20 55.56 150 85.23 Abnormal coagulation function Yes 9 25.00 13 7.39 5.331 .021 No 27 75.00 163 92.61 Recurrent hernia Yes 6 16.67 5 2.84 4.920 .027 No 30 83.33 171 97.16 Diabetes mellitus Yes 5 13.89 3 1.70 4.434 .231 No 31 86.11 173 98.30 Hypertension Yes 9 25.00 10 5.68 6.675 .010 No 27 75.00 166 94.32BMI = body mass index.
 Figure 3.:
Figure 3.: Clinical data and complications of patients undergoing laparoscopic inguinal hernia repair.
3.4. Binary Logistic regression analysis of risk factors for postoperative complicationsBased on the results of the univariate analysis of patients with and without complications, a binary Logistic regression analysis was implemented for the risk factors of BMI, intraoperative blood loss, intraoperative adhesions, abnormal coagulation function, recurrent hernia, and hypertension-related postoperative complications. The results showed that BMI, intraoperative blood loss, intraoperative adhesions, abnormal coagulation function, recurrent hernia, and hypertension were risk factors for postoperative complications of LIHR (P < .05), as shown in Table 2 and Figure 4.
Table 2 - Binary logistic regression analysis of risk factors for postoperative complications. Variable B SE Wald P OR 95% CI BMI 0.109 0.043 6.923 .006 5.201 0.816–6.965 Intraoperative blood loss 0.891 0.206 18.611 <.001 2.512 1.712–3.689 Medical history time 0.254 0.071 2.895 .321 0.553 0.222–0.886 Hernia sac management 0.760 0.721 1.168 .261 0.556 0.212–0.926 Intraoperative adhesions 1.062 0.446 8.236 .002 6.352 0.162–6.669 Abnormal coagulation function 0.709 0.135 27.598 <.001 2.063 1.563–2.668 Recurrent hernia 0.792 0.228 12.181 <.001 2.208 1.415–3.446 Hypertension 3.032 0.816 12.569 .000 3.652 0.009–6.32695% CI = 95% confidence interval, B = regression coefficient, BMI = body mass index, OR = odd ratio, SE = standard error.
 Figure 4.:
Figure 4.: Binary logistic regression analysis of risk factors for postoperative complications. BMI = body mass index.
4. DiscussionIn the Guidelines for the Diagnosis and Treatment of Inguinal Hernia in Adults in 2018, an inguinal hernia is defined as the degeneration of the transversus abdominis muscle in the weak area of the groin to form a defect in the brachiocephalic layer, which ultimately progresses to a hernia sac, and the hernia contents (mostly small bowel, followed by the greater omentum) are mostly formed by the entry of abdominal organs and tissues into the hernia sac, and the hernia content protrudes from the region of the inguinal defect onto the surface of the body, and the forming mass or bulge is referred to as an inguinal hernia.[11,12] Diagnosis of inguinal hernia is relatively simple, and sometimes a definitive diagnosis can be made simply based on the patient’s medical history and physical examination, but initial physical examination is difficult to determine the type of inguinal hernia in a patient.[13] At present, the treatment measures of inguinal hernia with a definite diagnosis include surgical treatment and conservative treatment, but surgical treatment is the most effective treatment for inguinal hernia; except for special patients (infants and children < 1 year old, elderly patients who are difficult to tolerate surgery, and those who are difficult to carry out surgery for concurrent illnesses), it is recommended to carry out surgery at an early stage, so as to avoid the subsequent progression of intestinal obstruction or intestinal necrosis.[14,15]
Laparoscopic surgery is currently widely applied in the surgical treatment of inguinal hernia, which can significantly shorten the postoperative activity time of patients and reduce the incision infection and recurrence rate,[16] but follow-up has indicated that there are still a large number of patients who experience adverse reactions such as chronic pain, which has a significant impact on the patient’s psychology and family economy. In this study, through the analysis of the data of patients who met the inclusion and exclusion criteria, it was found that 36 of the 212 enrolled patients with LIHR experienced complications, with an incidence rate of 16.98% (36/212), among which seroma and hematoma were the most common. A previous report[17] has pointed out that LIHR may cause damage to the inguinal lymphatic vessels of patients intraoperatively, resulting in postoperative lymphatic leakage, and if the patient has large and excessive free hernia sac, it may case hematoma due to postoperative local blood return obstruction. The authors of this study analyzed and believed that the results in this research were similar to the findings of other scholars,[18] suggesting a relative high incidence of postoperative complications in patients with LIHR, which needs to be taken into account by medical staff.
Furthermore, by grouping 212 enrolled patients according to the follow-up results, it was found that the patients in the complication group and the non-complication group exhibited significant differences in BMI, intraoperative blood loss, intraoperative adhesions, abnormal coagulation function, recurrent hernia, and hypertension. Further multivariate Logistic regression analysis found that BMI, intraoperative blood loss, medical history time, intraoperative adhesions, abnormal coagulation function, recurrent hernia, and hypertension were the risk factors for complications after LIHR.
According to the analysis from the authors of this paper, patients with high BMI mostly imply that they have poor surgical tolerance, and such patients are prone to comorbid diabetes or metabolic syndrome, and fat liquefaction is prone to occur in postoperative incisions, which in turn induces wound infections. By adopting grouping and comparison methods, Straton[19] found that overweight patients had a slower rate of incision healing and a higher incidence of incision infections after surgery compared with individuals with low BMI, and they believed that the reason may be related to abnormal hormone levels in obese individuals. Roadman et al[20] pointed out that obese patients had relatively higher levels of serum leptin and lipocalin, and these also exacerbated the occurrence and development of postoperative inflammation in patients, with the risk of inducing the emergence of chronic pain.
The results of this study also suggested that greater intraoperative blood loss may increase the incidence of postoperative complications. The authors of this study believed that the larger amount of intraoperative blood loss often represents more pronounced intraoperative trauma in patients, mostly implying a severe condition, which is also an important reason for the prolonged postoperative recovery process in patients. In addition, excessive intraoperative blood loss also increases the risk of events such as incomplete intraoperative hemostasis, increased volume of exudate fluid in the operative area, and accumulation of exudate, which may potentially increase the likelihood of postoperative hematoma in patients, and also increase the incidence of complications to some extent.
The presence of intraoperative adhesions excites the patient’s sympathetic nervous system, leading to hypofunction of the smooth muscle of their intestinal wall, affecting the secretion of intestinal secretions, and also leading to an increased risk of postoperative hematoma and myxodema in patients. For patients with coagulation disorders, appropriate coagulation medication is required, which increases the risk of acute postoperative urinary retention.[21] Through the implementation of follow-up of inguinal hernia patients, Liu et al[22] found that intraoperative adhesions could increase the difficulty of the surgery, significantly prolong the operative time, and even require additional resection operations, which significantly increased the trauma to the patient’s body, leading to an increase in the incidence of postoperative complications in patients.
Recurrent hernia suggests that patients have already undergone surgery or conservative treatment, and a secondary surgery can aggravate the damage to the original surgical site and increase events such as wound infection and bleeding, similar to the findings of Yamaguchi et al.[23] Finally, hypertension implies the presence of underlying diseases in patients, and these have been proven to be one of the important risk factors for complications after inguinal hernia surgery. As pointed out by Tripoloni et al,[24] hypertension affects several stages of surgical procedures; for instance, hypertension may increase intraoperative blood loss in patients, induce or exacerbate myocardial ischemia, and increase the incidence of events such as stroke and renal failure, etc., and thus, proper perioperative management of patients with hypertension is required to reduce the incidence of various complications.
5. ConclusionsIn conclusion, common complications in patients undergoing LIHR included seroma, hematoma, urinary retention, etc. BMI, intraoperative blood loss, intraoperative adhesions, abnormal coagulation function, recurrent hernia, and hypertension were the risk factors for complications after LIHR. This study provides a certain reference for the perioperative management of patients undergoing LIHR. However, it also has shortcomings such as small sample size and lack of long-term follow-up of patients. A large sample, multi-center and long-term follow-up study will be conducted in the future, so as to provide more detailed theoretical data reference for the perioperative management of patients with inguinal hernia.
Author contributionsConceptualization: Lexiang Chen, Mingfu Hu, Shanhu Huang.
Data curation: Mingfu Hu, Shanhu Huang.
Formal analysis: Mingfu Hu, Shanhu Huang.
Investigation: Mingfu Hu, Shanhu Huang.
Validation: Mingfu Hu, Shanhu Huang.
Writing – original draft: Lexiang Chen.
Writing – review & editing: Lexiang Chen.
References [1]. Dhanani NH, Bernardi K, Olavarria OA, et al. Port site hernias following laparoscopic ventral hernia repair. World J Surg. 2020;44:4093–7. [2]. Yamamoto K, Koda K. Favorable outcomes of transabdominal compared with transinguinal preperitoneal inguinal hernia repair. Minim Invasive Ther Allied Technol. 2022;31:962–8. [3]. Kakiashvili E, Bez M, Abu Shakra I, et al. Robotic inguinal hernia repair: is it a new era in the management of inguinal hernia? Asian J Surg. 2021;44:93–8. [4]. Pan C, Xu X, Si X, et al. Effect of complete reduction of hernia sac and transection of hernia sac during laparoscopic indirect inguinal hernia repair on seroma. BMC Surg. 2022;22:149. [5]. Lu Y, Chen DC, MacQueen IT. General surgery: management of postoperative complications following ventral hernia repair and inguinal hernia repair. Surg Clin North Am. 2021;101:755–66. [6]. Jan Z, Ali S, Ahmed N, et al. Comparison of common postoperative complications between lichtenstein open repair and laparoscopic transabdominal pre-peritoneal (TAPP) repair for unilateral inguinal hernia. Cureus. 2021;13:e17863. [7]. Miller BT, Prabhu AS, Petro CC, et al. Laparoscopic versus robotic inguinal hernia repair: 1- and 2-year outcomes from the RIVAL trial. Surg Endosc. 2023;37:723–8. [8]. Sürek A, Bozkurt MA, Ferahman S, et al. Laparoscopic total extraperitoneal inguinal hernia repair under epidural anesthesia versus general anesthesia. Surg Laparosc Endosc Percutan Tech. 2020;30:471–5. [9]. Lee SR. Adding laparoscopic iliopubic tract repair to transabdominal preperitoneal hernioplasty for treatment of recurrent inguinal hernia after totally extraperitoneal hernioplasty. J Laparoendosc Adv Surg Tech A. 2022;32:896–901. [10]. Gamborg S, Öberg S, Rosenberg J. Characteristics of groin hernia repair in patients without a groin hernia: a nationwide cohort study. Hernia. 2020;24:115–20. [11]. Kakizawa N, Tsujinaka S, Mizusawa Y, et al. Indications and outcomes of a hybrid method combining laparoscopic and anterior approaches for inguinal hernia repair. Cureus. 2022;14:e27117. [12]. Kojima S, Sakamoto T, Yajima K, et al. Open mesh removal combined with laparoscopic totally extraperitoneal inguinal hernia repair: a case report of a novel surgical technique for chronic postoperative inguinal pain. Asian J Endosc Surg. 2021;14:140–3. [13]. Fernandez-Alberti J, Iriarte F, Croceri RE, et al. Laparoscopic treatment (reTAPP) for recurrence after laparoscopic inguinal hernia repair. Hernia. 2021;25:1301–7. [14]. Smith L, Magowan D, Singh R, et al. Outcomes of primary and recurrent inguinal hernia repair with prosthetic mesh in a single region over 15 years. Ann R Coll Surg Engl. 2021;103:493–5. [15]. Xu EW, Mao ZQ, Wang HC, et al. Feasibility of laparoscopic indirect inguinal hernia repair with lateral umbilical fold covering internal inguinal ring combined with patch repair. Wideochir Inne Tech Maloinwazyjne. 2022;17:652–9. [16]. Trokovski N, Uchikov P, Yordanov E, et al. Advantages and disadvantages of laparoscopic inguinal hernia repair (hernioplasty). Folia Med (Plovdiv). 2022;64:61–6. [17]. Li J, Bao P, Shao X, et al. The management of indirect inguinal hernia sac in laparoscopic inguinal hernia repair: a systemic review of literature. Surg Laparosc Endosc Percutan Tech. 2021;31:645–53. [18]. Anitha B, Aravindhan K, Sureshkumar S, et al. The ideal size of mesh for open inguinal hernia repair: a morphometric study in patients with inguinal hernia. Cureus. 2018;10:e2573. [19]. Straton AA. The operative treatment of inguinal hernia in hospital. Hospital (Lond 1886). 1917;62:8. [20]. Roadman D, Helm M, Goldblatt MI, et al. Postoperative urinary retention after laparoscopic total extraperitoneal inguinal hernia repair. J Surg Res. 2018;231:309–15. [21]. Sun BJ. Study on the Risk Factors of Incarcerated Inguinal Hernia in Adults and the Efficacy of Different Surgical Modalities in the Treatment of Incarcerated Inguinal Hernia. (Article in Chinese). Lanzhou: Lanzhou University; 2022. [22]. Liu N, Greenberg JA, Xu Y, et al. Phone follow-up after inguinal hernia repair. Surg Endosc. 2021;35:5159–66. [23]. Yamaguchi N, Morioka D, Izumisawa Y, et al. A classification system specific for recurrent inguinal hernia following open hernia surgery. In Vivo. 2021;35:3501–8. [24]. Tripoloni DE, Canaro García MI, Cassani F, et al. Mesh repair for lateral inguinal hernias: a non-evidence-based practice. Hernia. 2021;25:1183–7.
留言 (0)