
Remember me

Since the invention of broad-spectrum antibiotics, the incidence of prostatic abscesses has decreased significantly.[1] Overall, the annual incidence of prostatic abscesses (PA) is 0.5% of all urological diseases, with mortality ranging from 1% to 16%.[2] Due to the rarity of its occurrence, no official guidelines for diagnosis and treatment have been developed.
Before the widespread use of antibiotics, Neisseria gonorrhoeae was the predominant pathogen (75%), but today gram-negative bacteria predominate.[1,3] Gram-negative Klebsiella pneumoniae (KP) commonly causes PA; however, its prevalence varies by geographic region. In southern Taiwan, KP is the predominant pathogen of PA,[4] whereas in South Korea, KP (17.3%) is the second most dominant bacterium, after E. coli (40.4%).[5] The incidence of KP-induced PA seems to be increasing, and related reports are also increasing. However, the pathogens are all carbapenem-sensitive KP, and there are no related reports of PA caused by carbapenem-resistant Klebsiella pneumoniae (CRKP). Here, we report a case of PA induced by CRKP.
2. Case reportA 21-year-old presented to the emergency department with a sudden onset of high fever (39.7°C), which decreased after self-administration of antipyretics. The patient experienced lower urinary tract symptoms such as frequency and urgency in the past month. Over 3 months previously, the patient was diagnosed with autoimmune encephalomyelitis and had a long-term indwelling catheter placed and long-term hormone treatment. After discharge, they continued to take prednisone acetate tablets 50 mg/day for more than 1 month.
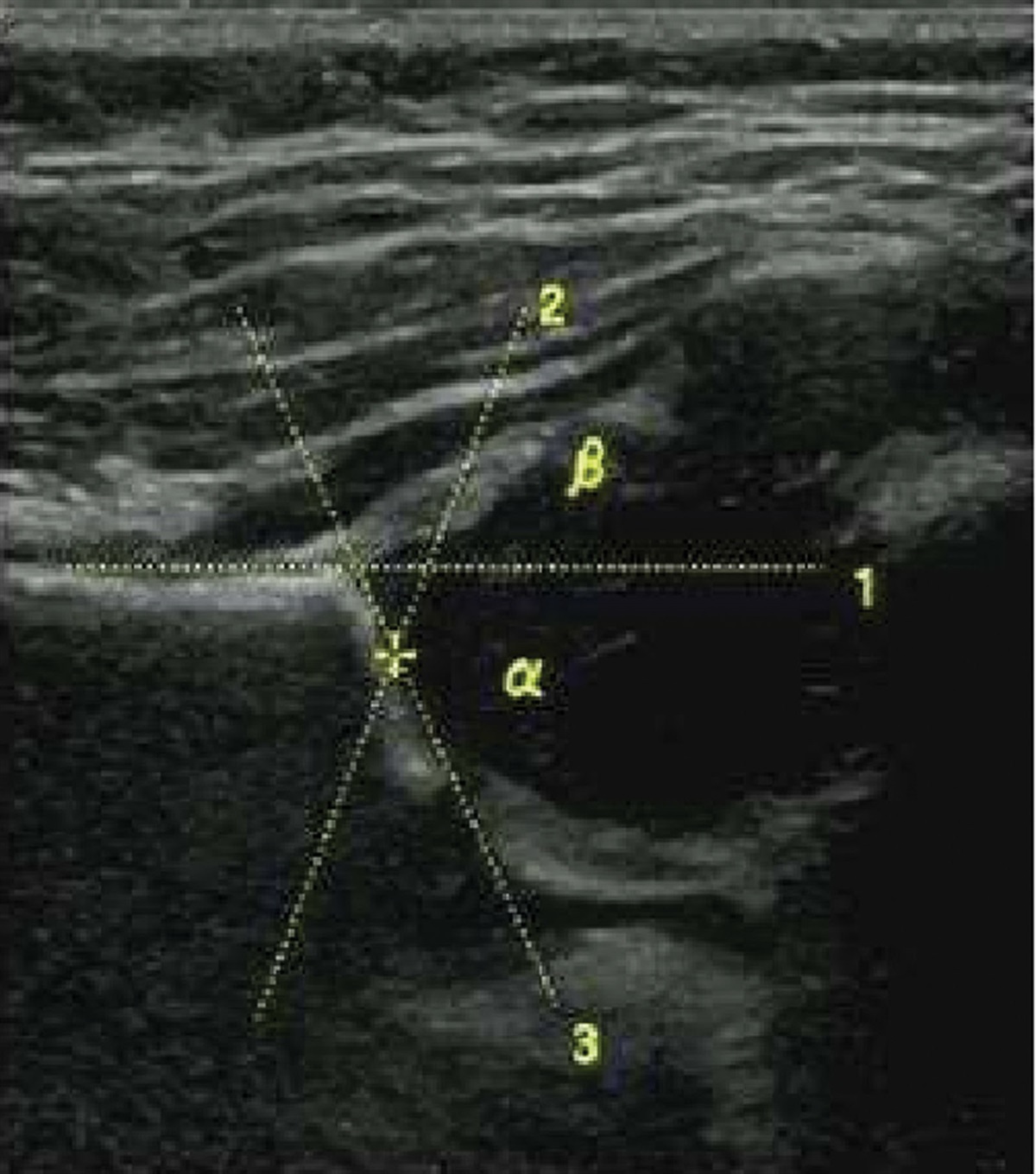
On this admission, the patient was conscious, with a blood pressure of 125/82 mm Hg, body temperature of 37°C, and heart rate of 98 beats/min. Anal palpation revealed a markedly elevated and tender prostate. Laboratory tests suggest an inflammatory reaction (Table 1). The subsequent pelvic magnetic resonance imaging showed a 2.1 × 2.9 × 2.8 cm hyperintense lesion on T1 and hyperintense T2, which was diagnosed as prostatic abscess (Fig. 1).
Table 1 - Laboratory results. Laboratory parameters (reference range) On admission 1st after surgery 3st after surgery 6st after surgery 9st after surgery 12st after surgery 16st after surgery 21st after surgery Leukocyte count (3.5–9.5 × 109/L) 9.04 11.71 9.13 20.07 13.29 10.32 8.75 7.38 Neutrophil count (1.4–7.12 × 109/L) 6.77 9.21 6.1 16.78 10.74 7.88 6.12 5.18 Neutrophil percentage (40%–75%) 74.90% 78.70% 66.80% 83.70% 80.90% 76.40% 73.00% 70.20% CRP (0–8 mg/L) 37.8 142 15.8 7.65 37.1 23.2 15.3 7.3 PCT (<0.5 ng/ml) 0.57 3.26 0.23 6.28 0.12 0.08 0.02 0.03 Urine leukocyte count (0–15/μL) 26.0 20.5 29.4 29.4 148.1 17.5 57.2 9.5CRP = C-reactive protein, PCT = procalcitonin.
 Figure 1.:
Figure 1.: Magnetic resonance imaging of the prostate showed a prostate abscess.
On the 8th day of admission, PA drainage was performed under general anesthesia to drain the abscess, relieve obstruction, and perform pus culture. That evening, the patient developed a high fever (38.9°C), chills, and hypotension (88/62 mm Hg). Laboratory tests showed elevated inflammatory markers (Table 1). We considered septic shock caused by postoperative hematogenous infection and empirically used imipenem for anti-infective treatment.
After 5 days of treatment, the patient still had recurrent low-grade fever without a significant decrease in inflammatory markers. Subsequent culture of urine and pus yielded KP, which was resistant to all injectable cephalosporins, aminoglycosides, carbapenems, piperacillin-tazobactam, and quinolones. Minocycline, tigecycline, and polymyxin were all potentially effective (Table 2). We then switched treatment to omalocycline. After 2 weeks of omalocycline treatment, the patient’s temperature returned to normal and the symptoms of urinary frequency and urgency completely resolved. Finally, the patient was discharged after recovery and did not experience recurrence during the 6-month follow-up period.
Table 2 - Antimicrobial susceptibility. Antibiotics MIC/KB Sensitivity Nitrofurantoin ≥128 R Gentamicin ≥16 R Ampicillin ≥32 R Cefuroxime ≥32 R Ceftazidime ≥32 R Cefepime ≥32 R Cefoxitin ≥32 R Ceftriaxone ≥64 R Piperacillin/tazobactam ≥128/4 R Ampicillin/sulbactam ≥64/32 R Meropenem ≥16 R Imipenem 4 R Compound sulfamethoxazole ≥64 R Levofloxacin ≥8 R Ciprofloxacin ≥4 R Cefoperazone/ Sulbactam ≥64/32 R Minocycline ≤4 S Polymyxin B 0.5 M Tigecycline ≤4 S Ceftolozane/tazobactam ≥8/152 RM = moderate, R = resistant, S = susceptible.
A prostatic abscess is an uncommon infection that is usually a complication of an ascending genitourinary infection caused by acute bacterial prostatitis or gram-negative bacilli in the intestine. Gram-negative bacteria are the predominant pathogens. Among these, KP is an important pathogen. The incidence of KP-induced PA seems to be increasing, and related reports are also increasing.[1,3] However, there are no related reports on PA caused by CRKP. To our knowledge, this is the first reported case of CRKP-induced PA.
The incidence of prostatic abscesses is low. However, under special circumstances, such as invasive procedures and immunosuppressed states, some patients may develop this disease. Risk factors for PA include diabetes mellitus, human immunodeficiency virus infection, prostatitis, urinary tract devices, indwelling catheters, voiding dysfunction secondary to obstruction, and neurogenic bladder.[6] Our case concurs that immunosuppression and long-term indwelling catheter use are risk factors for PA, and KP bacteremia may be a new risk factor for PA.
KP is ubiquitous in nature and is one of the most important opportunistic pathogens, causing a variety of human infections such as bloodstream infections, urinary tract infections, surgical site infections, and pneumonia.[7] Carbapenem-resistant strains are rapidly increasing owing to the spread of resistant plasmids and high-risk clones. Between 2001 and 2011, the prevalence of CRKP strains associated with central-line bloodstream infections in the United States increased from 1.6% to 10.4%.[8] In 2016, the prevalence of CRKP in different provinces of China ranged from 0.9% to 23.6%, with an average of 8.7%.[9] As antimicrobial resistance is increasing, various aspects of modern medicine are under threat, including oncology and surgical care. Additionally, long-term use of antimicrobial agents is widely accepted to treat CRKP. Long-term antibiotic treatment not only increases the treatment cost for patients but also increases the incidence of multi-drug resistant bacteria, which poses a dilemma for healthcare systems.
The incidence of CRKP in hospitalized patients is associated with immunosuppression, length of intensive care unit stay, severity of underlying disease, and previous exposure to different classes of antibiotics, including carbapenems, fluoroquinolones, cephalosporins, and glycopeptides.[10] Our case showed that immunosuppression, recent surgery, and previous exposure to different classes of antibiotics are risk factors for CRKP acquisition. The independent risk factors for CRKP exposure were prolonged hospital stay and sharing a room with a known carrier. Screening for CRKP at admission would protect against CRKP infection.[11] Thus, strict infection control is essential to prevent the spread of resistance.
KP is known for its multidrug resistance due to its ability to acquire resistance to different classes of antibiotics, including carbapenems, with limited availability of effective drugs. In fact, appropriate antibiotic treatment for CRKP remains an open question in clinical practice. In this case, we used omadacycline to treat CRKP bloodstream infection, the treatment effect was satisfactory, and no significant complications were noted.
Omadacycline, a tetracyclic antibacterial drug, is a novel aminomethylcycline antibiotic. It has a broad spectrum of antimicrobial activity against gram-positive and gram-negative bacteria, shows good antimicrobial activity against KP,[12] and shows activity against 2 of the most common tetracycline resistance mechanisms, namely ribosome protection and active efflux.[13] In addition, omadacycline has a lower plasma protein binding rate than tigecycline and a larger oral distribution volume than other tetracyclines, suggesting that omadacycline has higher tissue permeability and has advantages in the treatment of systemic infections.[14] Finally, its availability as an intravenous or oral formulation, long serum half-life, and once-daily administration are benefits of this next-generation tetracycline. It is worth noting that omadacycline is more cost-effective than tigecycline and polymyxin in China. Therefore, considering the efficacy and economic benefits of omadacycline, we believe that this is a better choice.
4. ConclusionPA is not commonly found, but some patients are more susceptible to this disease under certain host conditions. Immunodeficiency and invasive catheter use may be risk factors for PA and opportunistic bacterial infections. The use of omadacycline for the treatment of CRKP infections appears to be effective.
AcknowledgmentsThe authors would like to thank the patient and all the doctors and nurses participated in the case.
Author contributionsConceptualization: Wen-Qiang Zhou.
Data curation: Wen-Qiang Zhou.
Funding acquisition: Zhi Chen.
Investigation: Wen-Qiang Zhou.
Methodology: Wen-Qiang Zhou.
Project administration: Xue-Ju Cai.
Resources: Zhi Chen.
Supervision: Zhi Chen.
Validation: Zhi Chen, Xue-Ju Cai.
Writing – original draft: Wen-Qiang Zhou.
Writing – review & editing: Zhi Chen, Xue-Ju Cai.
References [1]. Weinberger M, Cytron S, Servadio C, et al. Prostatic abscess in the antibiotic era. Rev Infect Dis. 1988;10:239–49. [2]. Arrabal-Polo MA, Jimenez-Pacheco A, Arrabal-Martin M. Percutaneous drainage of prostatic abscess: case report and literature review. Urol Int. 2012;88:118–20. [3]. Collado A, Palou J, García-Penit J, et al. Ultrasound-guided needle aspiration in prostatic abscess. Urology. 1999;53:548–52. [4]. Liu KH, Lee HC, Chuang YC, et al. Prostatic abscess in southern Taiwan: another invasive infection caused predominantly by Klebsiella pneumoniae. J Microbiol Immunol Infect. 2003;36:31–6. [5]. Lee CR, Lee JH, Park KS, et al. Antimicrobial resistance of hypervirulent Klebsiella pneumoniae: epidemiology, hypervirulence-associated determinants, and resistance mechanisms. Front Cell Infect Microbiol. 2017;7:483. [6]. Ackerman AL, Parameshwar PS, Anger JT. Diagnosis and treatment of patients with prostatic abscess in the post-antibiotic era. Int J Urol. 2018;25:103–10. [7]. Podschun R, Ullmann U. Klebsiella spp as nosocomial pathogens: epidemiology, taxonomy, typing methods, and pathogenicity factors. Clin Microbiol Rev. 1998;11:589–603. [8]. Nordmann P, Cuzon G, Naas T. The real threat of Klebsiella pneumoniae carbapenemase-producing bacteria. Lancet Infect Dis. 2009;9:228–36. [9]. Hu F, Zhu D, Wang F, et al. Current status and trends of antibacterial resistance in China. Clin Infect Dis. 2018;67(suppl_2):S128–34. [10]. Schwaber MJ, Klarfeld-Lidji S, Navon-Venezia S, et al. Predictors of carbapenem-resistant Klebsiella pneumoniae acquisition among hospitalized adults and effect of acquisition on mortality. Antimicrob Agents Chemother. 2008;52:1028–33. [11]. Schwaber MJ, Carmeli Y. An ongoing national intervention to contain the spread of carbapenem-resistant enterobacteriaceae. Clin Infect Dis. 2014;58:697–703. [12]. Macone AB, Caruso BK, Leahy RG, et al. In vitro and in vivo antibacterial activities of omadacycline, a novel aminomethylcycline. Antimicrob Agents Chemother. 2014;58:1127–35. [13]. Villano S, Steenbergen J, Loh E. Omadacycline: development of a novel aminomethylcycline antibiotic for treating drug-resistant bacterial infections. Future Microbiol. 2016;11:1421–34. [14]. Rodvold KA, Burgos RM, Tan X, et al. Omadacycline: a review of the clinical pharmacokinetics and pharmacodynamics. Clin Pharmacokinet. 2020;59:409–25.
Comments (0)