
記住我
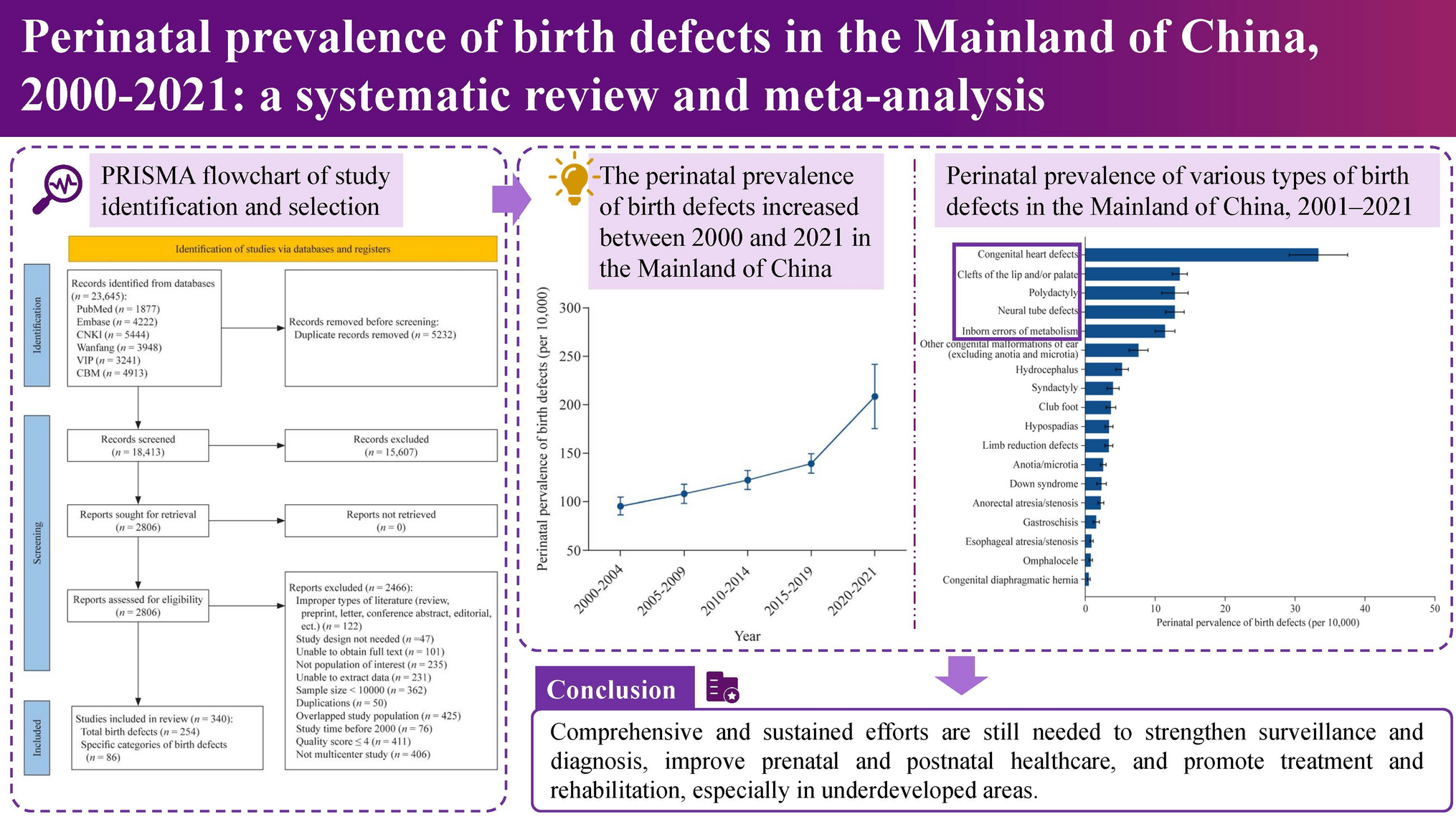
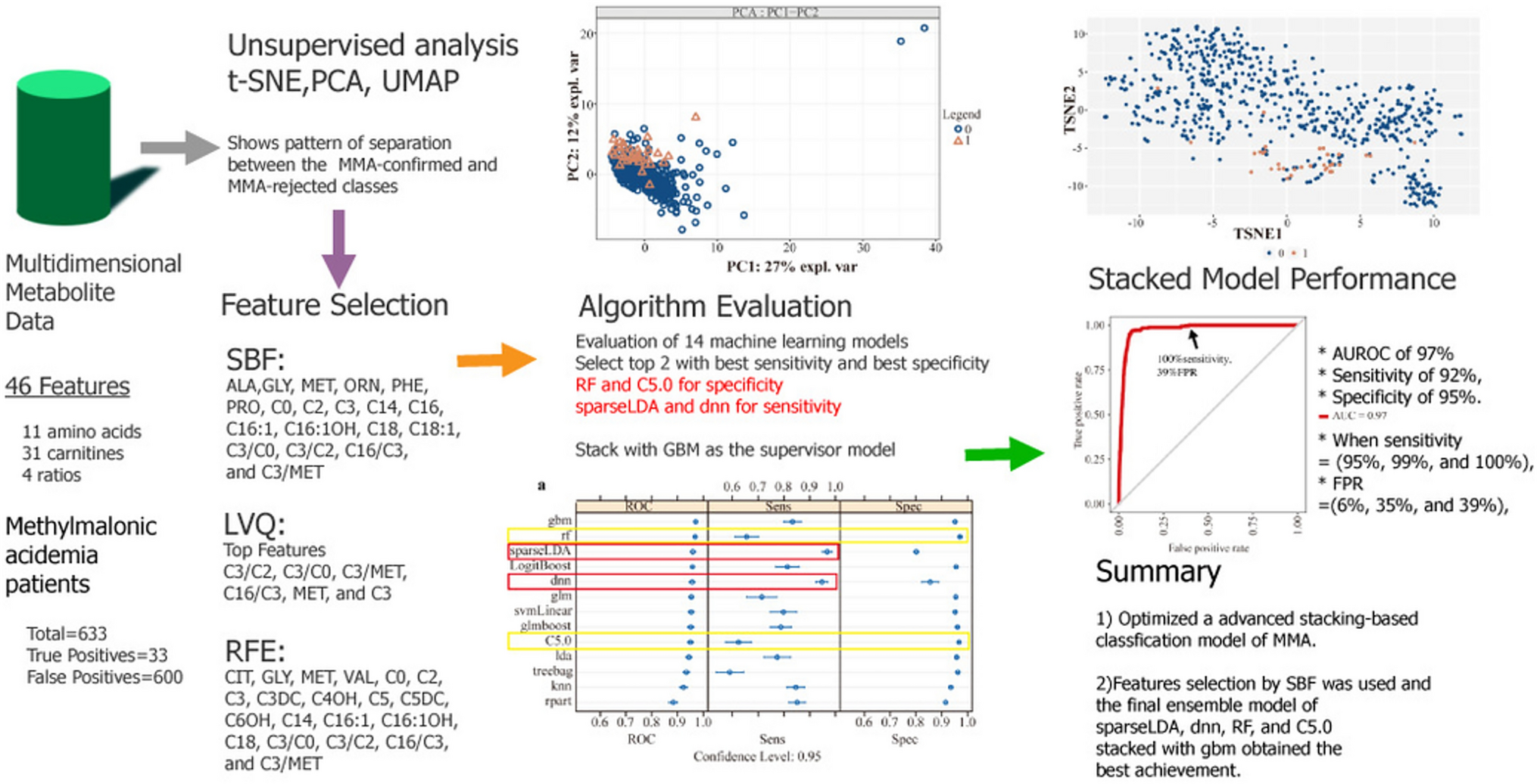


To explore the treatment effect of ACTH combined with MgSO4 for IESS patients, we conducted this retrospective study, as described in Fig. 1. A total of 1225 patients were extracted from the information systems of the two hospitals. After rigorous screening, patients who did not meet the inclusion criteria were excluded, along with those having duplicate hospitalization information (only including data from their first treatment) and patients with incomplete information. Ultimately, a total of 1101 individuals diagnosed with IESS were included in this study. They were categorized into two groups based on the treatment regimen administered during hospitalization: the ACTH combined with MgSO4 group (n = 814) and the ACTH monotherapy group (n = 287). While 96 patients did not finish the fortnight treatment, we finally obtained 744 patients receiving ACTH combined with MgSO4 treatment and 261 patients receiving ACTH treatment only. The clinical characteristics of these patients are shown in Table 1. The mean age of IESS patients was 10 months, and the age of onset was younger than 6 months. More than 90% of the enrolled patients were full-term infants, had flexor spasms and had no family history of NSD. We also noticed that more than half of the patients had taken more than two kinds of ASMs. Interestingly, most of the IESS patients had no epilepsy before the diagnosis of IESS and had no other diseases that may affect the nervous system, and the etiological classification of 54.4% of patients was unknown. It is notable that before PSM, the two groups had significant differences in some kinds of characteristics, such as sex, age of onset, number of ASMs used, family history of NSD, etiological classification and disease that affects the nervous system during the neonatal period. After PSM, the difference in all clinical characteristics disappeared, and 489 and 238 IESS patients received the combination treatment of ACTH combined with MgSO4 and ACTH, respectively.
Fig. 1
Flowchart of patient selection process. IESS infantile epileptic spasms syndrome, AED anti-epileptic drug, ACTH adrenocorticotropic hormone, MgSO4 magnesium sulfate
Table 1 Clinical characteristics of enrolled IESS patients before and after PSMEvaluation of the treatment efficacy of ACTH combined with MgSO4 and ACTH for IESS patientsNext, we evaluated the treatment effect of ACTH combined with MgSO4 and ACTH for IESS patients. In total, 744 IESS patients from the ACTH combined with MgSO4 group and 261 IESS patients from the ACTH group were enrolled in this study. As shown in Table 2, before treatment, the average seizure frequencies in the ACTH combined with MgSO4 and ACTH groups were 63.1 and 58.8 times per day, respectively, and there was no difference (P = 0.477). After two weeks of treatment, the average seizure frequency dropped to 10.8 and 25.5 times/day in the ACTH combined with MgSO4 and ACTH groups (P < 0.001), respectively. After treatment, 509 IESS patients from the ACTH combined with MgSO4 group and 144 IESS patients from the ACTH group achieved a reduction in seizure frequency of ≥ 50% compared to baseline and the resolution of hypsarrhythmia EEGs [68.4% (509/744), 95% confidence interval (CI) = 65.1%–71.8% vs. 55.2% (144/261), 95% CI = 49.1%–61.2%; P < 0.001]. Notably, complete response to treatment and successful cessation of seizures were observed in 444 IESS patients from the ACTH combined with MgSO4 group and 108 IESS patients from the ACTH group [59.7% (444/744) vs. 41.4% (108/261), P < 0.001]. No statistically significant difference was observed in the time between treatment initiation and seizure cessation, which was 7 and 8 days in the ACTH combined with MgSO4 and ACTH groups, respectively (P = 0.566) (Table 2). The mean baseline serum magnesium ion concentration in children in the ACTH combined with MgSO4 group was 0.90 ± 0.06 mmol/L, and the mean serum magnesium ion concentration after treatment was 1.02 ± 0.13 mmol/L. The difference in serum magnesium concentration before and after treatment was 0.11 ± 0.13 mmol/L, with a statistically significant difference (t = 23.33, P < 0.001, 95% CI = 0.10–0.12).
Table 2 Evaluation of the effect of ACTH combined with MgSO4 and ACTH treatment for IESS patientsAfter PSM, the responders in the ACTH combined with MgSO4 and ACTH groups also had significant differences. After treatment, 348 IESS patients from the ACTH combined with MgSO4 group and 128 IESS patients from the ACTH group achieved a reduction in seizure frequency of ≥ 50% compared to baseline and the resolution of hypsarrhythmia EEGs [70.8% (348/489), 95% CI = 66.7%–74.8% vs. 53.8% (128/238), 95% CI = 47.4%–60.2%; P < 0.001]. In addition, 381 IESS patients in the ACTH combined with MgSO4 group and 141 IESS patients in the ACTH group had hypsarrhythmia EEGs that disappeared [77.9% (381/489) vs. 59.2% (141/238), P < 0.001]. The average seizure frequency dropped from 60.2 times/day to 10.1 times/day in the ACTH combined with MgSO4 groups compared to 59.1 to 26.2 times/day in the ACTH group (P < 0.001). Similarly, complete response to treatment and successful cessation of seizures were observed in 305 IESS patients from the ACTH combined with MgSO4 group and 95 IESS patients from the ACTH group [62.4% (305/489) vs. 39.9% (95/238), P < 0.001]. The average baseline serum magnesium ion concentration in children was 0.91 ± 0.06 mmol/L, and the average serum magnesium ion concentration after treatment was 1.01 ± 0.12 mmol/L. The difference in serum magnesium concentration before and after treatment was 0.11 ± 0.13 mmol/L, and the difference was still statistically significant (t = 18.08, P < 0.001, 95% CI = 0.09–0.11). This result indicated that the concentration of magnesium ions in the body of IS children significantly increased after treatment with ACTH combined with MgSO4. Interestingly, even in children with refractory IESS, ACTH combined with MgSO4 treatment demonstrated more significant therapeutic efficacy. After treatment, 191 refractory IESS patients from the ACTH combined with MgSO4 group and 64 refractory IESS patients from the ACTH group achieved a reduction in seizure frequency of ≥ 50% compared to baseline and the resolution of hypsarrhythmia EEGs [65.2% (191/293) vs. 48.9% (64/131), P = 0.002] (Table 2).
Multivariate analysis for ACTH combined with MgSO4 treatmentSubsequently, a statistical analysis was performed to identify factors within the ACTH combined with MgSO4 group that could potentially influence treatment outcomes. The dependent variable was treatment outcome, while baseline quantitative and qualitative data were considered independent variables, and logistic regression was employed for evaluation. Before PSM, two factors exhibited statistical significance, including the lead time to treatment and the number of ASMs taken before ACTH combined with MgSO4 treatment. We found that patients who had taken ≥ 2 types of ASMs before ACTH combined with MgSO4 treatment had a 63.4% increased risk of ineffective treatment compared to those with < 2 types (P = 0.012, 95% CI = 1.116–2.394). Furthermore, the risk of ineffective treatment increased by 4.3% as the lead time to treatment increased by an additional month (P = 0.04, 95% CI = 1.002–1.087). However, after conducting PSM and reperforming logistic regression analysis, only these two factors remained statistically significant. The risk of ineffective treatment increased by 67.9% in the patients who had taken ≥ 2 types of ASMs before ACTH combined with MgSO4 treatment compared to those who had taken < 2 types of ASMs (P = 0.026, 95% CI = 1.064–2.649). Additionally, the risk of ineffective treatment increased by 5.7% if the lead time to treatment increased by 1 month (P = 0.043, 95% CI = 1.002–1.115).
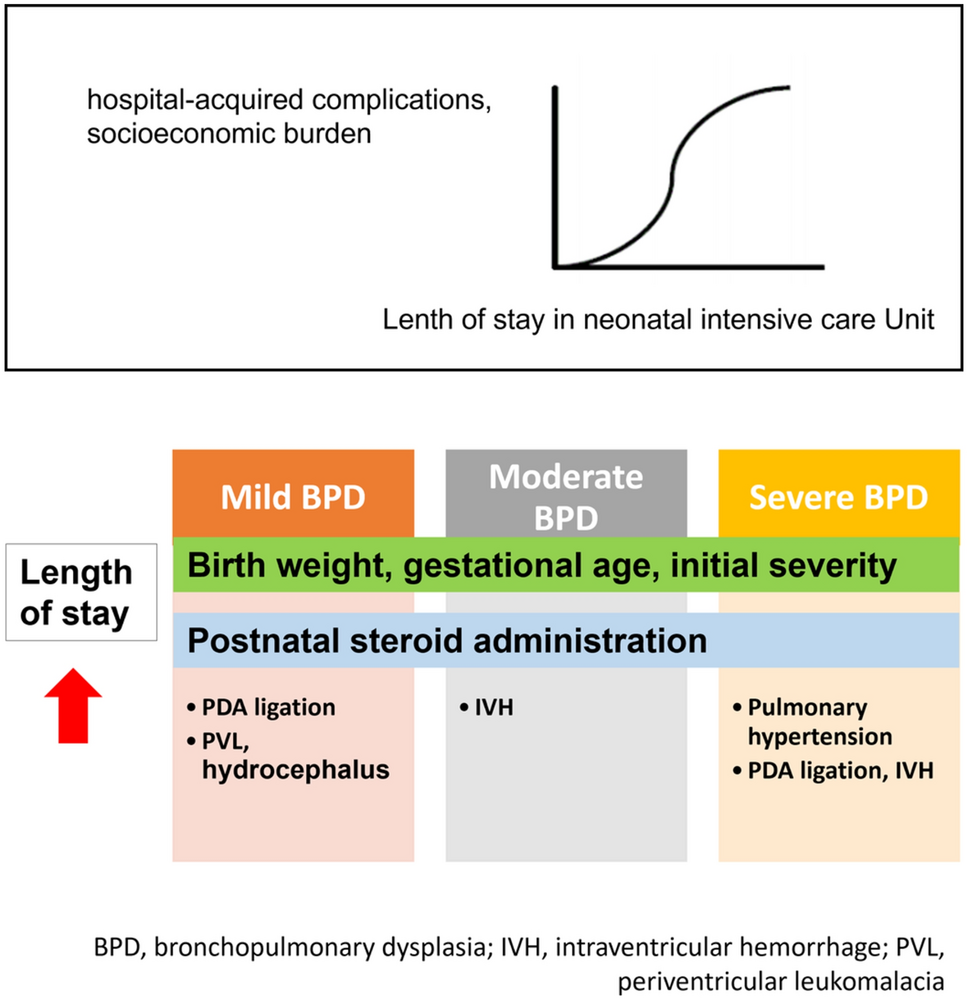
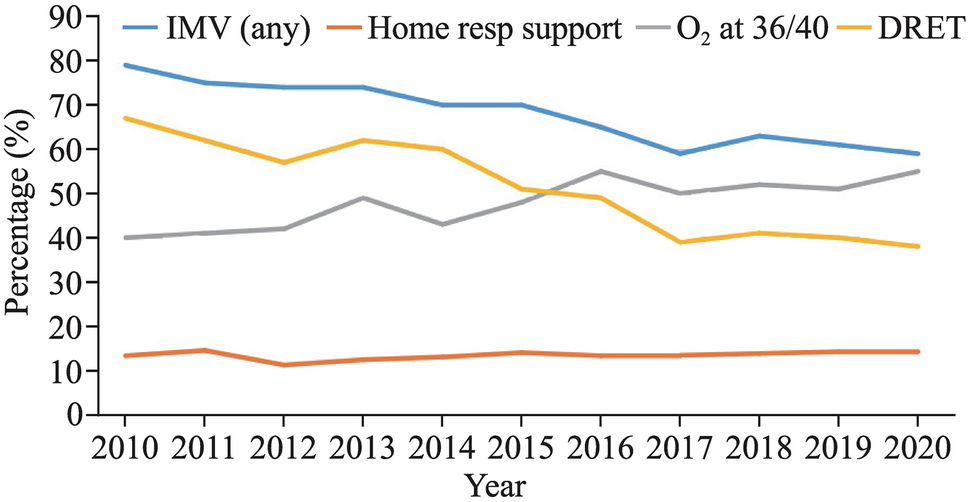
Subgroup analysis of the lead time to treatment and outcomeSubsequently, subgroup analysis was conducted based on the lead time to treatment and treatment outcomes. Patients were categorized into four subgroups according to their lead time (0 <–≤ 1 month, 1 <–≤ 3 months, 3 <–≤ 6 months, > 6 months). Following ACTH combined with MgSO4 treatment, the response rates of patients in these subgroups were 77.3%, 75%, 65%, and 61.8%, respectively. There was a statistically significant difference in response rates observed across these subgroups (χ2 = 12.693, P = 0.005). Patients with a lead time to treatment of less than 3 months exhibited a significantly better response to ACTH combined with MgSO4 treatment than those who had a lead time to treatment exceeding three months (P < 0.05). After performing PSM matching, the response rates in the four subgroups treated with ACTH combined with MgSO4 were 84.8%, 77.2%, 62.8%, and 64.3%. Significant differences persisted among these groups (χ2 = 13.539, P = 0.004) (Fig. 2a). Similar trends were also evident in the ACTH treatment group (Fig. 2b).
Fig. 2
Lead time to treatment and response rate. a The response rates of IESS patients in different lead time to treatment groups after PSM who underwent ACTH combined with MgSO4 treatment; b the response rates of IESS patients in different lead time to treatment groups after PSM who underwent ACTH treatment. PSM propensity score matching, IESS infantile epileptic spasms syndrome, ACTH adrenocorticotropic hormone, MgSO4 magnesium sulfate
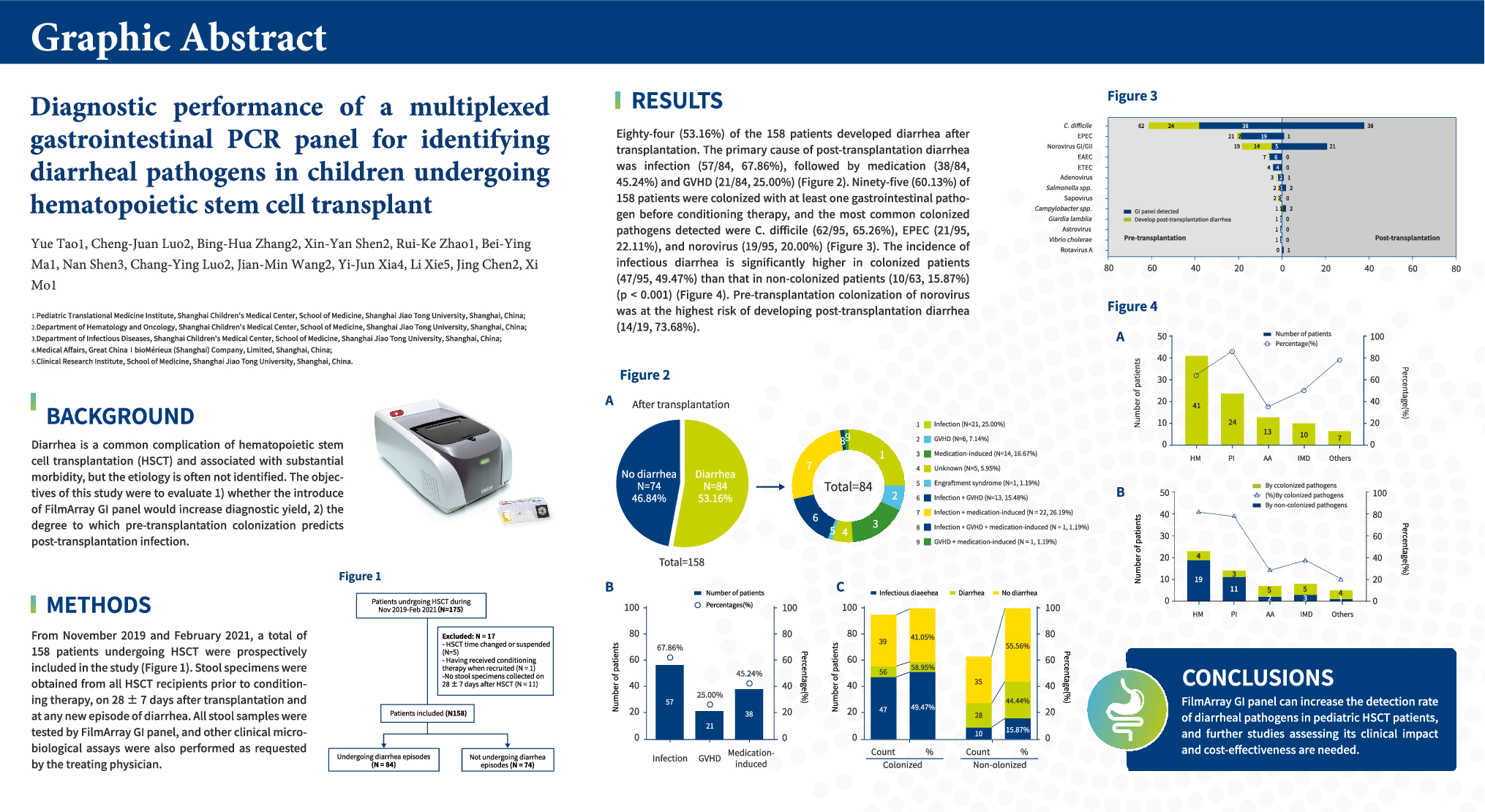
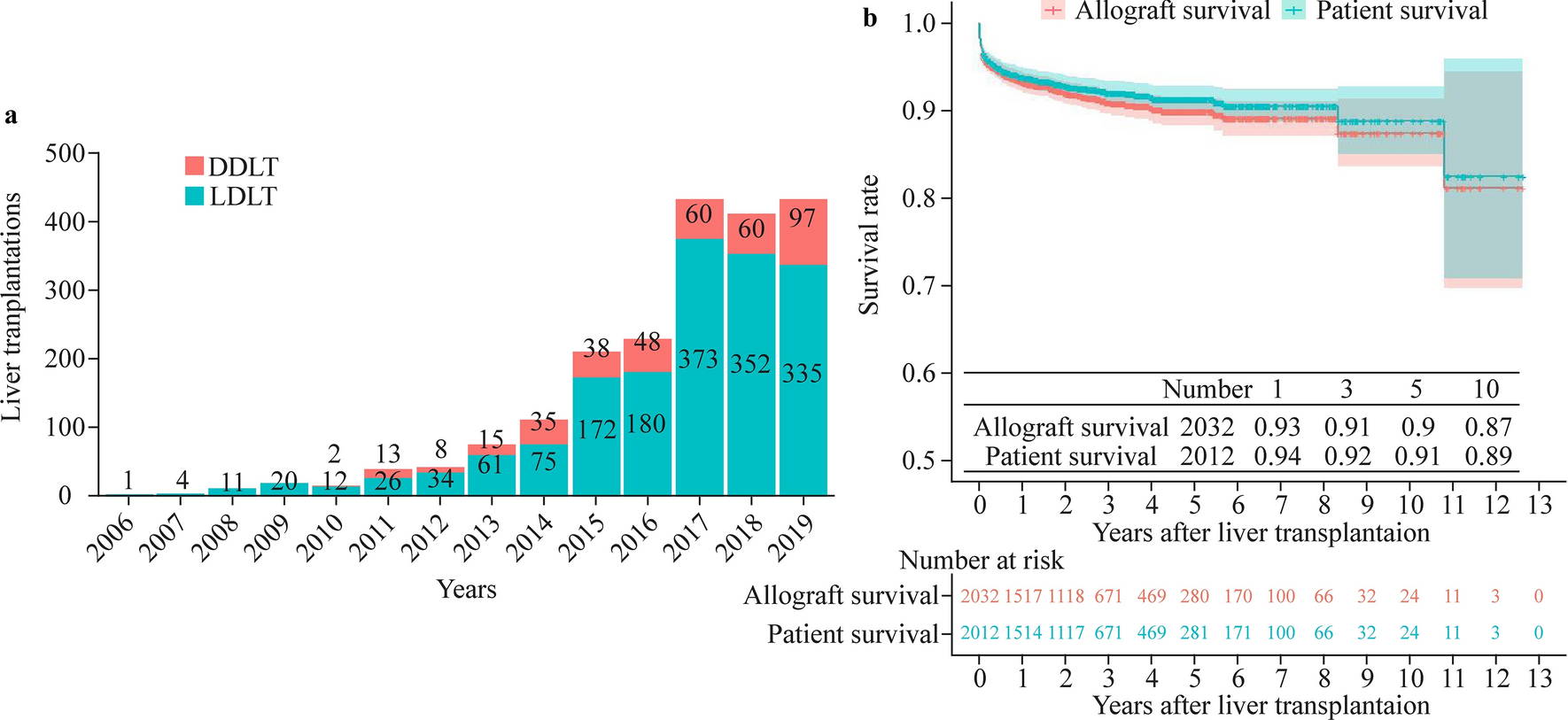
Multivariate analysis of factors influencing the treatment effect of hypsarrhythmia EEGTo further investigate additional factors that may influence the resolution rate of hypsarrhythmia EEG, we conducted a logistic regression analysis with the hypsarrhythmia EEG results as the dependent variable and treatment protocol and baseline quantitative and qualitative data as independent variables. Interestingly, following PSM, we found that only the treatment protocol emerged as a significant factor influencing the resolution rate in hypsarrhythmia EEG. After treatment, the risk of children in the ACTH treatment group still exhibiting hypsarrhythmia EEG was 1.502 times higher compared to those in the ACTH combined with MgSO4 treatment group (P < 0.001, 95% CI = 1.776–3.524). This finding suggests that ACTH combined with MgSO4 may have an advantage in improving hypsarrhythmia EEG. The alterations in hypsarrhythmia EEG before and after treatment with ACTH combined with MgSO4 in IESS patients are depicted in Fig. 3a and b.
Fig. 3
The alterations in hypsarrhythmia EEG before and after treatment of two IESS patients. a A female infant aged 6.8 months who was diagnosed with IESS and presented significantly hypsarrhythmia EEG patterns (chaotic, high amplitude, excessive slowing, multifocal epileptiform discharges). After receiving treatment with ACTH combined with MgSO4, the hypsarrhythmia EEG was effectively resolved; b a male infant aged 7.3 months who was also diagnosed with IESS and exhibited hypsarrhythmia EEG. However, after undergoing a combined treatment protocol, he demonstrated substantial improvement toward normalization. IESS infantile epileptic spasms syndrome, EEG electroencephalography, ACTH adrenocorticotropic hormone, MgSO4 magnesium sulfate
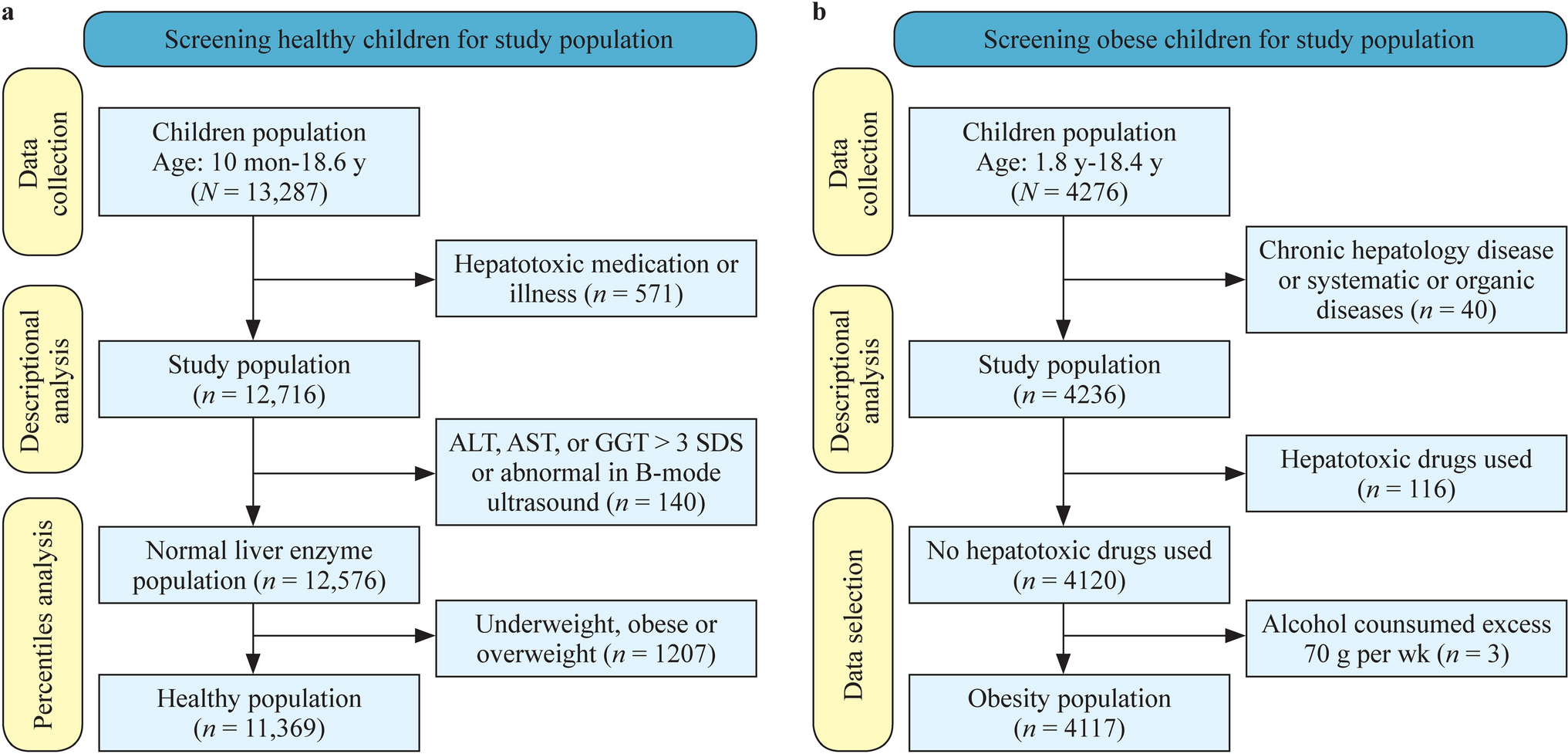
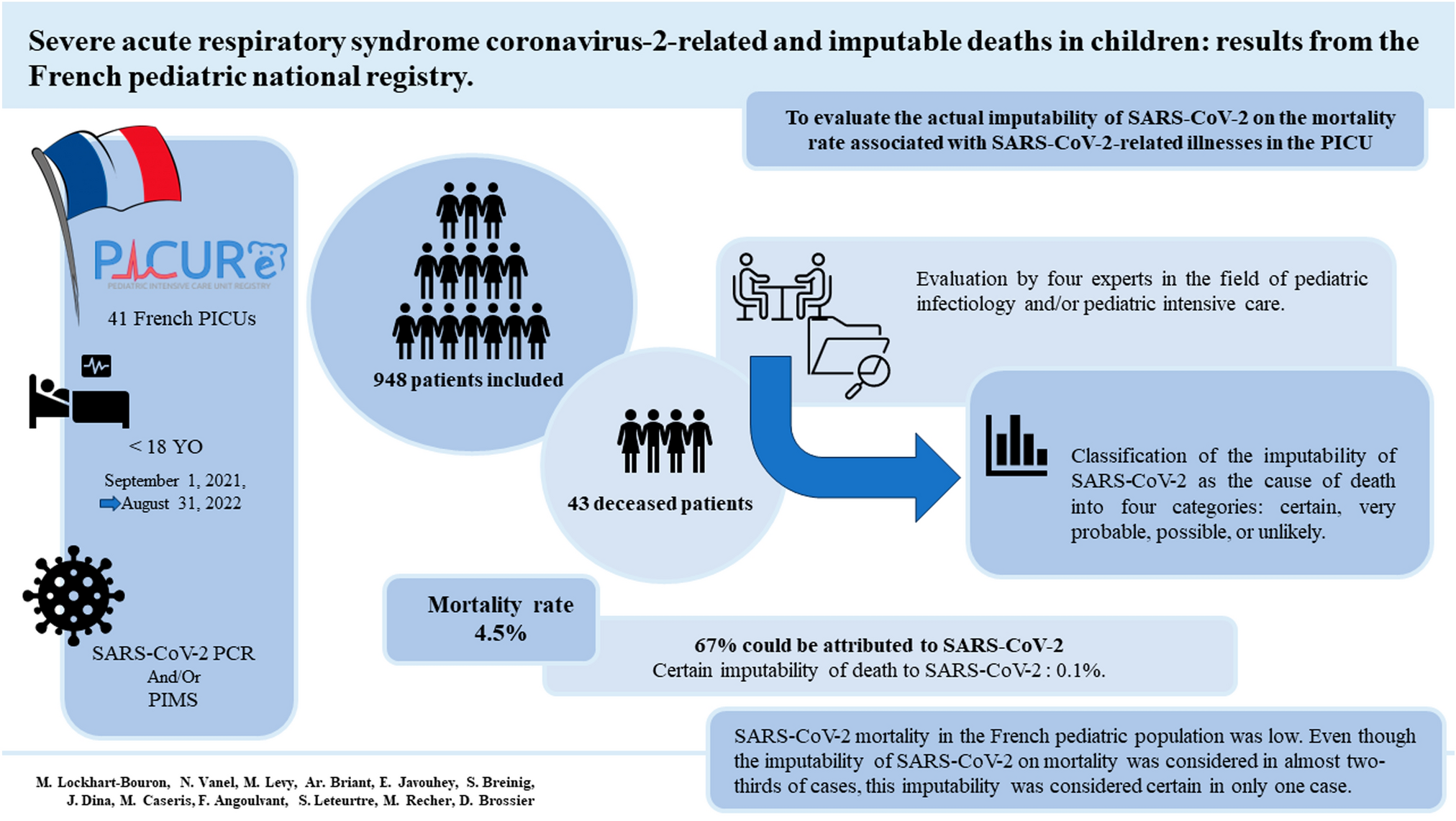
Analysis of the pathogeny causesWe subsequently conducted a statistical analysis of the etiology of the 1005 IESS patients included in the study. Among these IESS patients, 45.57% (458/1005) had identifiable causes. Of these patients with a clear cause, 84.28% (386/458) were attributed to structural/metabolic factors, while the remaining 15.72% (72/458) were due to genetic factors (Table 1). Subgroup analysis of the 386 IESS children attributed to structural/metabolic factors revealed that neonatal hypoglycemic encephalopathy accounted for the highest proportion at 25.13% (97/386), followed by cerebral dysplasia at 23.32% (90/386), neonatal hypoxic-ischemic encephalopathy at 22.54% (87/386), focal cortical dysplasia at 8.81% (34/386), and tuberous sclerosis at 3.37% (13/386) (Fig. 4a). Additionally, among the 72 IESS patients with genetic causes identified, disease-associated gene mutations were detected in 67 cases, and disease-associated chromosomal microdeletions were detected in five cases (Supplementary Table 1). The top ten most frequently observed gene variations are shown in Fig. 4b. Cyclin-dependent kinase-like 5 gene mutation was detected in five cases as the most prevalent alteration. We also observed mutations in genes such as aristaless-related homeobox, potassium voltage-gated channel subfamily Q member 2, NF, Reelin, ryanodine receptor type 3, alpha-II-spectrin, and syntaxin-binding protein 1 among IESS patients.
Fig. 4
Summary of causes. a Top 10 structural/metabolic causes of enrolled IESS patients; b number of IESS patients caused by genetic variations. IESS infantile epileptic spasms syndrome, CDKL5 cyclin-dependent kinase like 5, ARX aristaless-related homeobox, KCNQ2 potassium voltage-gated channel subfamily Q member 2, RELN Reelin, RYP3 ryanodine receptor type 3, SPTAN1 alpha-II-spectrin, STXBP1 syntaxin-binding protein 1, IQSEC2 IQ motif and SEC7 domain containing protein 2, SCN1A sodium voltage-gated channel alpha subunit 1, SCN2A sodium voltage-gated channel alpha subunit 2
Analysis of the incomplete respondersAfter two weeks of treatment, 71 patients had resolution on hypsarrhythmia EEG but had a reduction rate of seizure frequency less than 50% or even worsened. There were another 152 patients who had no resolution on hypsarrhythmia EEG but had a reduction rate of seizure frequency equal to or greater than 50%. The clinical characteristics of these patients can be seen in Table 3. After PSM, we selected 48 patients from the group with resolved hypsarrhythmia EEG but persistent seizure frequency and 103 patients from the group with unresolved hypsarrhythmia EEG but significantly reduced seizure frequency. In the group with resolved hypsarrhythmia EEG but persistent seizure frequency, the average age of patients was 10.8 months, more boys (64.6%), the average age of onset was 4.8 months, the average lead time to treatment was 6.1 months, an average of 2.2 types of ASMs were taken before receiving treatment, the pathogeny cause of half of them could be characterized, and 72.9% of the patients received the combination treatment. In the group with unresolved hypsarrhythmia EEG but significantly reduced seizure frequency, the average age was 9.9 months, more boys (68.9%), the average age of onset was 4.5 months, the average lead time to treatment was 5.4 months, the pathogeny cause for 35% of the patients could be characterized, and 68% of the patients received the combination treatment. The statistical analysis did not identify any factors that may cause significant differences between the two groups.
Table 3 Clinical characteristics of incomplete respondersSafety analysisAmong the 814 IESS patients receiving ACTH combined with MgSO4 treatment and 287 IESS patients receiving ACTH alone treatment (including those patients who did not complete the full two weeks of treatment) (Fig. 1), a total of 397 patients (256 patients receiving ACTH combined with MgSO4 treatment and 181 patients receiving ACTH treatment) had adverse reactions/events (Table 4). The most common adverse reaction was infection caused by low immunity due to ACTH administration, with 115 cases in the ACTH combined with MgSO4 treatment group and 94 cases in the ACTH treatment group (P < 0.001). Electrolyte disorders and hypertension were also significantly different between the two groups (Table 4). No statistically significant differences were observed between the two groups in terms of external heart rate, bradycardia, anemia, constipation, intussusception, anal fissure, or abnormal eye movements, which should be considered adverse events. In addition, serious adverse complications, including infection, diarrhea, allergic rash or allergic reaction, irritability and arrhythmia, occurred in 72 patients treated with ACTH combined with MgSO4 and 23 patients treated with ACTH alone (Table 4). Among these events, only infection (P = 0.045) and hypertension (P = 0.025) were significantly different between the two groups, and no deaths occurred during the treatment. Overall, the incidence of adverse reactions/events in the ACTH combined with MgSO4 group was 31.4%, which was lower than that in the ACTH group (P < 0.001). The total incidence of infection in the ACTH combined with MgSO4 group was 21.1%, which was lower than that in the ACTH group (P < 0.001). The total incidence of hypertension in the ACTH combined with MgSO4 group was 0.5%, which was also lower than that in the ACTH group (P < 0.001).
Table 4 Number of IESS patients with adverse reactions to the treatment
留言 (0)