



記住我




Over the past decade, there has been an observed increase in the prevalence and incidence of Inflammatory Bowel Diseases (IBD), specifically Crohn’s Disease (CD) and Ulcerative Colitis (UC) (Molodecky et al., 2012; Roy and Dhaneshwar, 2023). According to a recent epidemiological study conducted by Ng et al. (2017), IBD affects over 0.3% of people in North America and Europe. It is a group of gastrointestinal disorders with chronic inflammation. The cause of IBD is not fully understood but is believed to be a combination of genetic and environmental factors. Factors such as diet, use of antibiotics, and socioeconomic status can influence persistent immune-mediated inflammation in the intestines. (Manichanh et al., 2012; Çavdar and Çavdar, 2023). UC is a chronic gastrointestinal disorder characterised by chronic inflammation of the colorectal mucosa, resulting in non-specific inflammatory changes. The aetiology of this condition remains uncertain, and its conversion into cancer is not easily treatable. Ungaro et al. (2017) conducted epidemiological research which substantiated the global increase in the prevalence of UC. It is a condition caused by a combination of genetic, immune, microbial, and environmental factors. It involves persistent inflammation of the mucosal lining, affecting the rectum and proximal colon segments. The exact mechanisms behind UC development are not fully understood, but it is widely recognised that environmental factors, host genetics, a dysregulated immune system, and microbial dysbiosis play crucial roles. (Ananthakrishnan, 2015).
According to the study conducted by Higuchi et al. (2012), there is evidence to suggest that the adoption of Westernised diets and lifestyles can heighten the susceptibility of genetically predisposed individuals to IBD. Environmental factors encompass various aspects, such as residing in industrialised nations, urbanised settings, and regions situated at higher latitudes. In addition to infections and smoking, other factors also play a role in the pathogenesis of IBD. Patients frequently need lifelong medication, which is the main purpose of therapy, both to persuade clinical remission and to conserve it for a long period. According to the Global Burden of Disease Study, the estimated global prevalence of Crohn’s disease was approximately 6.8 million individuals, while ulcerative colitis affected approximately 10 million individuals. (Alatab et al., 2020).
These data suggest that, in addition to finding effective therapeutic approaches to advance IBD patients’ quality of life and lower healthcare system costs, it is crucial to better understand the factors involved in the development of IBD. Costs of IBD management have increased significantly in the past five years due to different therapeutic interventions and disease characteristics. Patients face increased healthcare utilisation, out-of-pocket expenses, and reduced productivity, necessitating the implementation of cost-effective solutions. (Park et al., 2020) Recent research suggests that microbiota can be therapeutically effective in treating IBD. The gut microbiome influences host processes and can mitigate inflammation. Various therapeutic approaches, including prebiotics, probiotics, and synbiotics, have been developed to alter and restructure the gut microbiome. (Britton et al., 2021) The most common strains currently available as probiotics and possessing beneficial health effects are Enterococcus faecium, Bifidobacterium, Bacillus, Saccharomyces boulardii (S. boulardii) and Lactobacillus strains. Prebiotics like fructo-oligosaccharides (FOS), isomalto-oligosaccharides (IMO), and xylooligosaccharide (XOS) are studied for their potential benefits on stool volume, constipation relief, and faecal acidity, with easily metabolised by Bifidobacteria and other microorganisms. (Guarino et al., 2020).
2 Understanding ulcerative colitisUlcerative colitis is a chronic inflammatory disorder of the gastrointestinal tract characterised by a progressive decline in health. UC is characterised by inflammation of the mucosal lining, typically confined to the colon and rectum. On the other hand, CD involves inflammation that extends through the entire thickness of the gastrointestinal tract, with a predilection for the ileum, terminal ileum, and colon. The CD is often associated with additional inflammatory conditions outside of the intestines. According to Çavdar and Çavdar (2023), the medical characteristics encompass symptoms such as hemorrhagic diarrhoea, weight loss, fatigue, and abdominal pain. Additionally, certain individuals may develop extra-intestinal manifestations associated with IBD, such as primary sclerosing cholangitis, skin lesions, or joint complications (Judge and Lichtenstein, 2001). The impact of UC on a global scale has been evaluated, revealing that it affects a population of approximately 5 million individuals. UC is characterised by recurring episodes of inflammation in the mucosal layer of the colon, which alternate between periods of relapse and remission. In ulcerative colitis, inflammation is typically confined to the mucosal surface. The disorder originates in the rectum and typically progresses proximally throughout the entirety of the colon. To date, a conclusive therapeutic approach for UC remains elusive, and the currently available interventions primarily focus on sustaining remission (Roy and Dhaneshwar, 2023).
Conventional therapies for UC consist of pharmacological interventions involving the use of various agents, including azathioprine, aminosalicylates, and corticosteroids. These treatments aim to induce remission, prevent relapses, promote mucosal healing, and ultimately reduce the need for colectomy in individuals diagnosed with UC. In recent times, advancements in medical treatments have been influenced by the utilisation of agents such as monoclonal antibodies that specifically target proinflammatory cytokines, adhesion molecules, T-cell activation, and agents that promote the production of anti-inflammatory cytokines, such as IL-10 (Interleukin) and Transforming Growth Factor (TGF). However, the administration of these medications in the context of ulcerative colitis is associated with a distinct set of systemic and localised adverse effects experienced by individuals. These include but are not limited to, symptoms such as headache, abdominal pain, nausea, cramping, loss of appetite, vomiting, and rash. In addition, it is not recommended to use corticosteroids for an extended period due to their potential to induce glucose intolerance, osteoporosis, myopathy, and increased vulnerability to infections. These adverse effects raise significant concerns regarding the safety profile of corticosteroid usage (Mowat et al., 2011). Similarly, the expenses associated with these promising therapeutic approaches are substantial, considering the increasing prevalence and persistent nature of IBD. Histological examinations conducted on patients with UC have revealed the presence of impaired intestinal epithelial barrier function. However, the significance of this dysfunction with the pathology of UC remains uncertain. Patients diagnosed with UC exhibit changes in the function of the epithelial barrier, impaired function of tight junctions, and reduced secretion of mucin-2. Nevertheless, the exact relationship between these abnormalities and chronic inflammation, accompanied by heightened cytokine production, remains uncertain. Heller et al. (2005) conducted a study that yielded evidence indicating that the overexpression of IL-13 plays a pivotal role in the disruption of tight junctions within the intestinal mucosal layer of individuals who have been diagnosed with active UC. The dysfunction of the barrier function in individuals diagnosed with UC has been linked to a heightened absorption of luminal antigens and an elevated susceptibility to bacterial infiltration in the underlying mucosa. Extensive research has provided comprehensive insights into the dysregulation of the intestinal immune system in individuals afflicted with UC. Dendritic cells (DCs) are known to have a pivotal role in the augmentation of UC patients, thus signifying the substantial contribution of these cells in the initiation and perpetuation of inflammatory processes (Hart et al., 2005).
3 Conventional treatments for UCConventional therapies play a pivotal role in the management of ulcerative colitis and the mitigation of associated symptoms. The objective of these treatments is to manage inflammation, initiate and sustain remission, and enhance the overall quality of life for patients. The Selecting Therapeutic Targets in IBD (STRIDE)-II statement was revised by the International Organisation for the Study of IBD to enhance the treatment of IBD in adults and children. The revised statement identified several goals at different timeframes. In the short term, achieving symptomatic remission and normalising C-reactive protein levels were prioritised. In the intermediate term, reducing calprotectin levels was identified as a target. Lastly, in the long term, the goals included achieving endoscopic healing and standardising the quality of life for individuals with IBD (Im et al., 2018; Turner et al., 2021). The subsequent therapies listed are commonly employed conventional treatments for ulcerative colitis.
3.1 AminosalicylatesAminosalicylates, alternatively referred to as 5-aminosalicylic acid (5-ASA) drugs, encompass a class of pharmaceuticals that possess the capability to mitigate inflammation within the gastrointestinal tract. These therapeutic agents function by specifically targeting the mucosal lining of the colon and rectum, which is the site of inflammation. Aminosalicylates are offered in diverse formulations, encompassing oral pharmaceuticals, rectal suppositories, and enemas. Corticosteroids are frequently employed as an initial therapeutic approach for individuals with mild to moderate ulcerative colitis, effectively managing symptoms and sustaining periods of remission. The class of medications known as 5-ASA-based drugs includes sulfasalazine, olsalazine, Mesalazine and balsalazide. These medications are widely recognised for their efficacy, safety, and affordability in the treatment of IBD, particularly UC (Sood et al., 2019).
3.2 CorticosteroidsCorticosteroids, such as prednisone and budesonide, exhibit potent anti-inflammatory properties and have demonstrated efficacy in promptly alleviating symptoms associated with moderate to severe ulcerative colitis exacerbations. These medications function through the inhibition of the immune system and the mitigation of inflammation within the colon. Corticosteroids are commonly prescribed for a limited duration to induce remission or manage acute symptoms. The avoidance of prolonged corticosteroid use is typically recommended due to the potential for significant adverse effects. According to Wild et al. (2003) and Waljee et al. (2016), these interventions effectively decrease intestinal inflammation by promptly reducing intestinal permeability, suppressing the production of Tumour necrosis factor (TNF) and inhibiting Nuclear factor-κB (NF-κB).
3.3 ImmunomodulatorsImmunomodulators represent a category of pharmaceutical agents that exert a modulatory or regulatory effect on the immune system. Patients who exhibit poor responses to aminosalicylates or corticosteroids are frequently prescribed these medications. Additionally, they may be used as a maintenance therapy to mitigate the occurrence of flare-ups., mercaptopurine (MP), Azathioprine (AZT) and methotrexate (MTX) are among the immunomodulators commonly employed in the treatment of ulcerative colitis. These pharmaceutical agents function by inhibiting the immune response and diminishing inflammation within the colon. According to Singh et al. (2022), in cases where patients with IBD do not respond to 5-ASA drugs and are reliant on or unresponsive to corticosteroids, it is advised to utilise conventional immunomodulators such as 6-MP, AZT, and MTX to maintain remission.
3.4 Biologic therapiesBiologic therapies are a relatively new class of pharmaceutical interventions that specifically target specific molecules or cells involved in the inflammatory pathway of ulcerative colitis. These interventions are usually recommended for people with moderate-to-severe symptoms who have not responded to conventional treatment. Biological therapeutics, such as anti-tumour necrosis factor (TNF) agents (e.g., adalimumab & infliximab) or integrin receptor antagonists (e.g., vedolizumab), function by inhibiting specific proteins or cells involved in the inflammatory processes taking place in the gastrointestinal tract. In contemporary medical practice, infliximab and adalimumab are the prevailing anti-tumour necrosis factor-alpha (TNF- α) agents that are frequently employed. The administration of these medications occurs through intravenous and subcutaneous routes, respectively. According to Seo and Chae (2014), clinical trials have provided evidence supporting the efficacy of infliximab and adalimumab in the treatment of moderate-to-severe UC.
3.5 Surgical interventionsSurgical interventions are necessary for treating ulcerative colitis when severe symptoms arise, complications arise, or conventional treatments are ineffective. Proctocolectomy involves removing the colon and rectum, with or without an ostomy. This procedure has high efficacy in eradicating the afflicted colon, providing patients with a prolonged period of remission. Treatment selection depends on the severity and scope of ulcerative colitis, as well as individual patient factors and preferences. (Kuhn and Klar, 2015).
4 Antibiotics used in UC treatmentRifaximin modifies gut microbiota for small intestinal bacterial overgrowth and hepatic encephalopathy, while antibiotics aim to manipulate intestinal flora, potentially disrupting IBD progression. In their study, Khan et al. (2011) conducted a meta-analysis that examined the findings of 10 randomised controlled trials (RCTs) focused on the utilisation of antibiotics in patients diagnosed with active CD. Additionally, the study also included nine RCTs that investigated the impact of antibiotic usage in individuals with UC. Antibiotics significantly impact remission and disease severity in UC and CD. Rifamycin derivatives are effective in treating active CD. However, results vary due to different trials involving rifaximin, fluoroquinolones, macrolides, and anti-tuberculosis antibiotics. (Steinhart et al., 2002).
5 The role of gut microbiota in UCThe gut microbiota, an important group of microorganisms that live in the digestive tract, is correlated to several diseases, including ulcerative colitis. The composition and function of the microbiota in the gut have both been shown to be susceptible to change, as recent research has shown. The gastrointestinal tract of a neonate does not initially contain any microorganisms but is eventually colonised by bacteria that come from the mother and the environment. (Dominguez-Bello et al., 2010). According to Vyas and Ranganathan (2012), the number of bacterial cells present on and within the entire body of an adult human is approximately ten times greater than the total number of human cells. The complexity and diversity of the human microbiome are considerable. The composition and quantity of anatomical features vary across different regions of the gastrointestinal tract, ranging from the nasal and oral cavities to the distal segments of the colon and rectum. The composition and complexity of the gut microbiota exhibit variability during the transition of infants from a liquid diet to solid foods. The alterations in dietary patterns during adulthood play a substantial role in shaping the composition of the gut microbiota. Metagenomic techniques based on 16S ribosomal RNA sequence have improved our understanding of microbial communities in the gastrointestinal tract. This approach reveals that 90% of the bacterial population is attributed to Bacteroidetes and Firmicutes. (Mariat et al., 2009; Hu and Gubatan, 2023).
5.1 Dysbiosis in UCDysbiosis in the gut microbiota is the root cause of ulcerative colitis. This condition is characterised by a decrease in commensal bacteria such as bifidobacteria and Lactobacilli and an increase in pathogenic bacteria such as Escherichia coli and Fusobacterium. The imbalance that can result from dysbiosis can put a person at risk for several different diseases, including IBD and irritable bowel syndrome. Additionally, it has the potential to bring about unanticipated outcomes, such as the activation of an HIV infection or the development of autoimmune diseases. (Liu et al., 2016).
5.2 Impaired gut barrier functionThe gut microbiota and intestinal epithelial cells collaborate to establish a defensive barrier aimed at impeding the infiltration of pathogens and toxins into the bloodstream. The integrity of the barrier function in ulcerative colitis is compromised, resulting in heightened permeability of the intestinal lining. The presence of dysbiosis in individuals with ulcerative colitis has been observed to have a detrimental effect on the integrity of the gut barrier. This compromised barrier allows for the infiltration of pathogenic bacteria and their associated metabolic by-products into the intestinal mucosa, subsequently eliciting an immune response. This phenomenon gives rise to atypical immune-inflammatory responses, including inflammation, allergies, and autoimmune disorders, which are facilitated by molecular mimicry and dysregulated T-cell reactions. According to the study conducted by Barnaba and Sinigaglia, 1997, it was found that the maintenance of intestinal homeostasis and the differentiation between harmful pathogens and beneficial commensal microbes heavily rely on the Treg/TH17 ratio, which represents the equilibrium between regulatory T cells (Tregs) and T helper type 17 cells (TH17). This regulation is strongly linked to the gut microbiota, as commensal microorganisms, including Firmicutes, Bacteroides fragilis and Bifidobacterium infantis promote the expansion of Treg cells, specifically FOXP3-expressing Treg and IL-10-producing Treg lymphocytes. Foxp3+ regulatory T cells play a crucial role in gut immunity and physiology, inducing intestinal tolerance and defending the host against harmful dietary antigens, commensal microorganisms, and pathogens. They also facilitate local tissue repair and maintain the integrity of the epithelial barrier, making them essential non-immune cells in the gastrointestinal tract. (Cosovanu and Neumann, 2020).
5.3 Immune system dysregulationThe gut microbiota exerts a substantial impact on the maturation and modulation of the immune system. Individuals diagnosed with UC exhibit an atypical immune response towards the gut microbiota, which is distinguished by an intensified activation of the immune system and the persistence of inflammatory processes. The dysregulation of the immune system can sustain the ongoing cycle of inflammation and subsequent tissue damage in the colon, thereby playing a role in the advancement of ulcerative colitis. The dysregulation of the immune response in the intestinal region is a crucial factor in the development of IBD, involving various molecules such as cytokines. In a recent study conducted by Kmiec et al. (2017), it was demonstrated that there is a correlation between the innate immune response and the promotion of gut inflammation in patients with IBD. The mucosa of patients with UC exhibits an altered equilibrium between regulatory T-cells and effector T-cells, including Th1, Th2, and Th17 cells. Evidence suggests that there is a correlation between UC and an a typical type 2 immune response, which is mediated by non-classical natural killer T-cells that produce IL-5 and IL-13. Previous studies have demonstrated that IL-13, which is secreted by specific subsets of NKT cells, plays a crucial role in exerting cytotoxic effects on epithelial cells. These effects include the induction of apoptosis and alterations in the composition of tight junction proteins (Fuss and Strober, 2008; Heller et al., 2008). Poggi et al. (2019) demonstrated a correlation between the exacerbation of pathology and the presence of supplementary inflammatory cytokines, including TNF, IL-1, IL-6, and IL-9.
5.4 Role of short-chain fatty acidsShort-chain fatty acids (SCFAs) are one of many metabolites produced by the gut microbiota during the fermentation of dietary fibres,exhibit anti-inflammatory properties. These fatty acids, typically not exceeding six carbon atoms, are derived from prebiotic or microbially fermentable carbohydrates like inulin, polysaccharides, and resistant starch. (Dalile et al., 2019) Butyrate, acetate, and propionate are examples of SCFAs that play important roles in intestinal health.The observed effects include acceleration of the regeneration and healing process of intestinal epithelial cells, augmentation of mucus production, and maintenance of appropriate pH levels within the intestine. Moreover, they hinder the attachment of pathogenic microorganisms to enterocytes. Acetate is commonly utilised as a cellular energy substrate for the growth and maintenance of muscle tissue and colonic cells. Butyrate exhibits a variety of beneficial effects on the host, such as strengthening metabolism, modulating the host’s immune system, and facilitating anti-inflammatory mechanisms. As a result, it attracts considerable attention. (Guarino et al., 2020) One of the hallmarks of UC is a decrease in SCFAs production, which contributes to an already severe inflammatory response and jeopardises the GI tract’s overall health. Because of this decline in SCFAs producers, it is common to find lower levels of SCFAs in faeces taken from people with inflammatory IBD. In a study of people with UC, Machiels et al. (2013) found lower levels of acetate and propionate in their faeces but not butyrate. When studying faecal samples from people with IBD Huda-Faujan et al. (2010) found lower levels of butyrate and propionate. Recent research findings indicate notable disparities in gut microbial species, microbial diversity and metabolic pathways between individuals diagnosed with IBD and healthy individual. (Lavelle and Sokol, 2020)
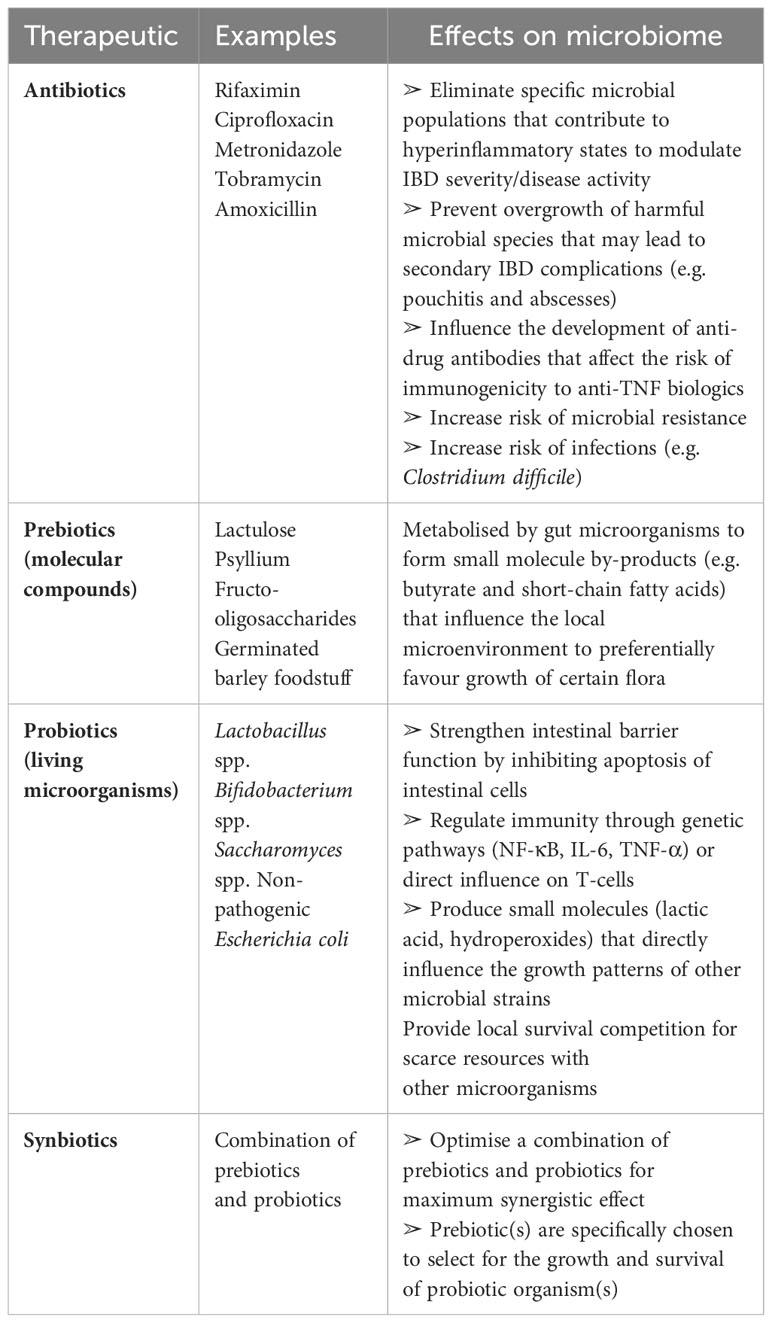
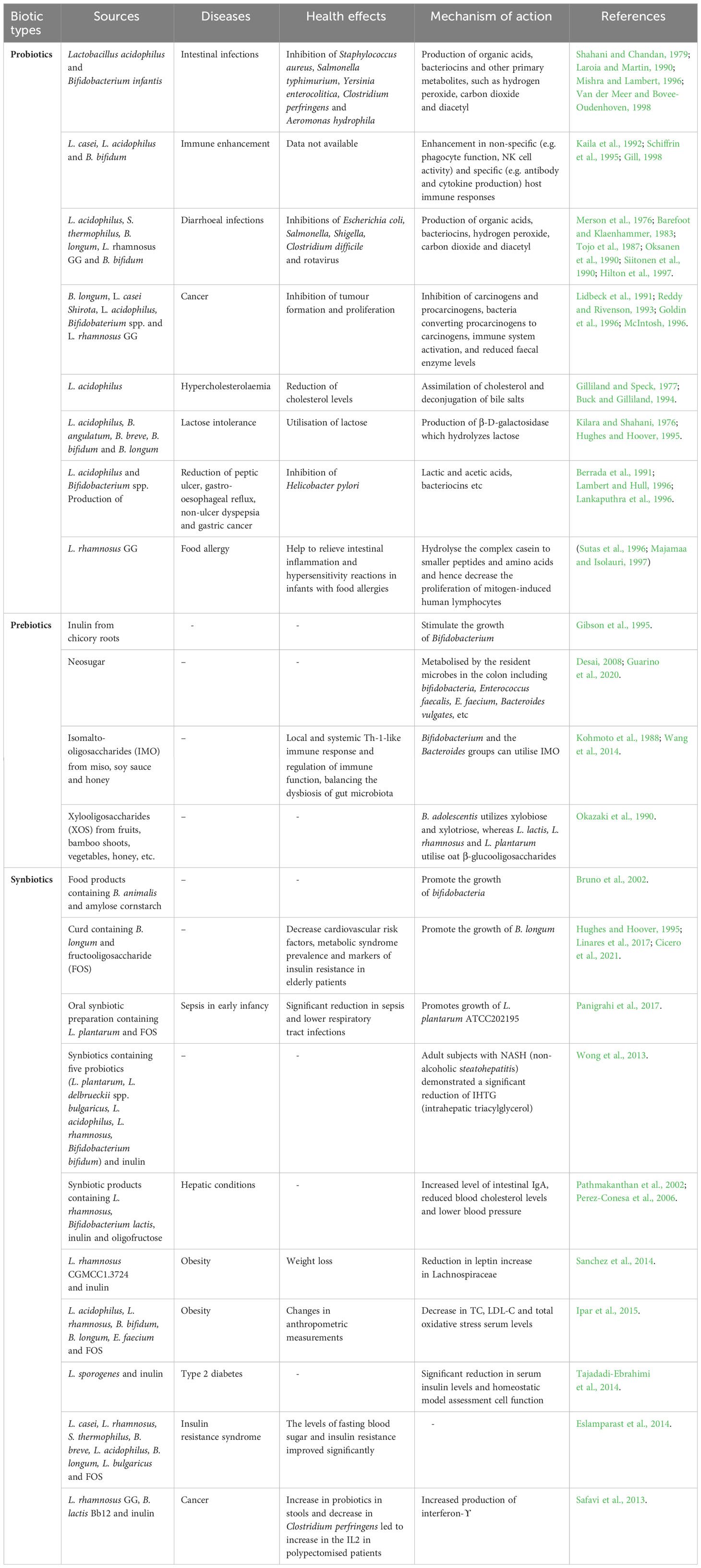
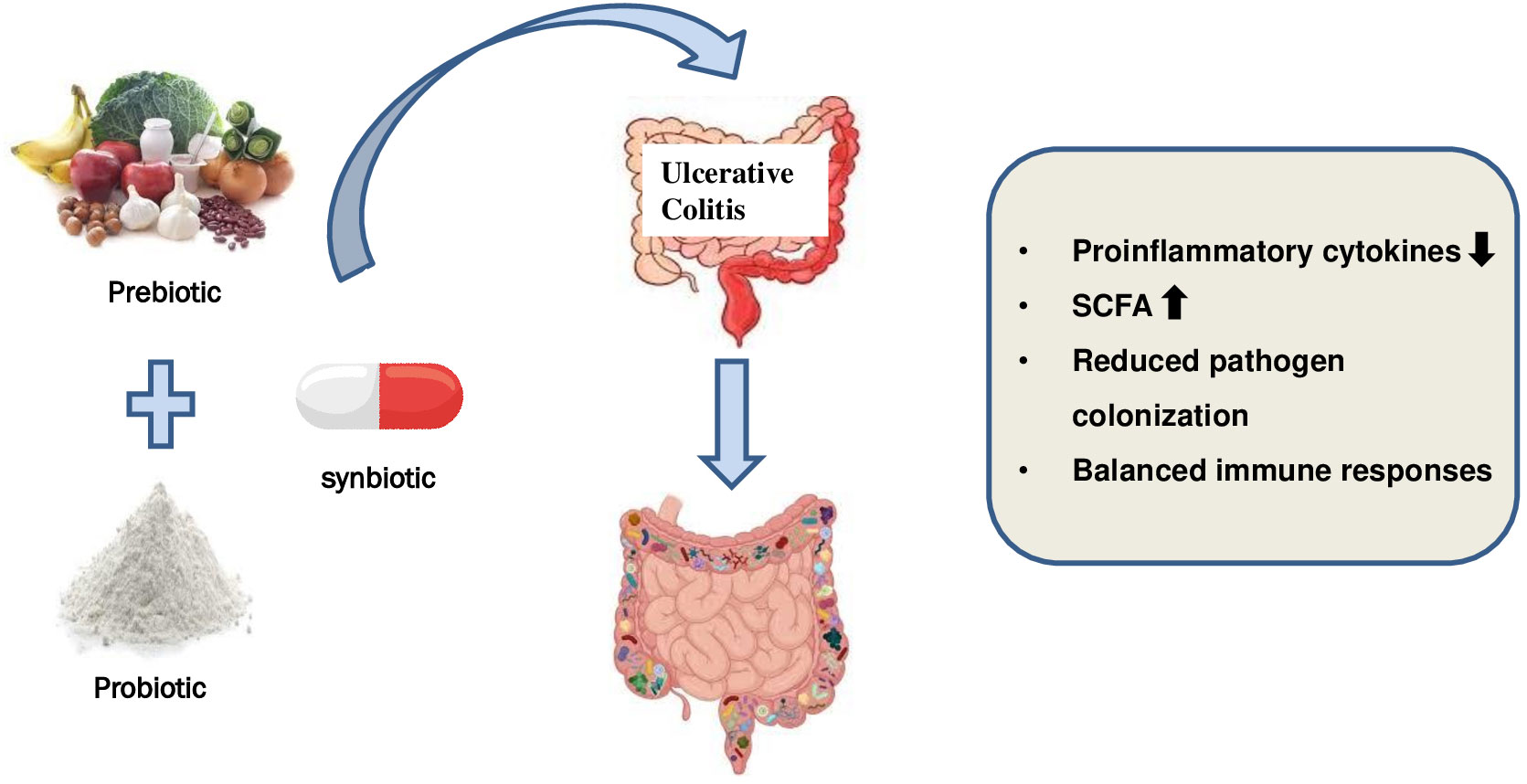
5.5 Potential therapeutic strategiesDue to the significant impact of the gut microbiota on ulcerative colitis, there is a growing interest in the development of effective strategies aimed at modulating the microbiota to restore equilibrium and improve disease outcomes. This involves the utilisation of probiotics, which are live beneficial bacteria that can be employed to reinstate the equilibrium of microorganisms in the gastrointestinal tract. Prebiotics, classified as dietary fibres that possess the ability to selectively enhance the proliferation of advantageous bacteria, can additionally be employed to enhance the growth of beneficial microorganisms. In addition, the utilisation of synbiotics, a combination of probiotics and prebiotics, may exhibit synergistic outcomes in the restoration of equilibrium within the gut microbiota (Hu and Gubatan, 2023). The present review provides an overview of the existing microbiome-centred therapeutic strategies employed in the management of IBD, as outlined in Table 1.
Table 1 Summary of current microbiome-based therapeutic strategies in IBD.
6 Probiotics: restoring balance in the gutProbiotics can be traced back to ancient civilisations when humans first began eating fermented foods as part of their regular diet. It was hypothesised by Elie Metchnikoff that the beneficial bacteria found in yoghurt could improve the health of the gut microbiome. Mackowiak (2013) presented the concept of probiotics for the first time. These microorganisms can positively modulate the composition of the gut microflora and reduce the presence of pathogenic bacteria that release harmful compounds within the human gastrointestinal tract. In previous studies, a range of microorganisms have been employed for disease management, thereby giving rise to the term “probiotics”. Probiotics, derived from Greek, refer to living, non-pathogenic organisms with beneficial effects on hosts. Vergin, in 1954, coined the term “probiotic” to compare the harmful effects of antibiotics on intestinal microbiota with the beneficial effects of some beneficial bacteria. The term “probiotic” was subsequently redefined by Lilly and Stillwell as a biologically active product produced by a microorganism that enhances the growth of another microorganism. As a result, the term was subsequently defined by Fuller (1989) as non-pathogenic microorganisms that, when ingested, have a beneficial impact on the health or physiology of the host. The most recent definition proposed by the FDA and WHO in collaboration is that of a live microorganism that, when administered in adequate quantities, confers a health advantage to the host. Several probiotic microorganisms are commonly utilised, species of Bifidobacterium and Lactobacillus, have been reported to be the predominant and subdominant groups among gut microbes, respectively (Casellas et al., 2007; Markowiak and Śliżewska, 2017). Bacterial organisms capable of forming spores, primarily belonging to the genus Bacillus, are prevalent in this context (Derikx et al., 2016; Jin et al., 2023).
Probiotics are incorporated into various food products, particularly fermented dairy products, either individually or in conjunction with other strains. Continuously, novel genera and strains of probiotics are being discovered through increasingly sophisticated and targeted research endeavours. VSL#3 is a combination of eight distinct probiotic strains, exhibiting high strain specificity and variability in benefits across different patient groups. Probiotic products can consist of a solitary strain or a mixture of two or more strains, with the effectiveness of multi-strain probiotics demonstrated in controlled studies. (Chapman et al., 2011). The study of probiotics, particularly Lactobacilli, has experienced significant growth over the past twenty years. This is evident from the substantial increase in research articles published on the topic. Specifically, while there were approximately 180 research articles available between 1980 and 2000, the number of articles on the probiotic Lactobacillus exceeded 5700 between 2000 and 2014. According to a study published in PubMed in 2014, the effectiveness of the probiotic strain Lactobacillus was investigated. The characteristics of an ideal probiotic strain are depicted in Figure 1.
Figure 1 Characteristics of an ideal probiotic strain.
Probiotics act against intestinal diseases through various processes, including colonisation, which enhances their efficacy. They produce inhibitory constituents like organic acids, fatty acids, hydrogen peroxide, SCFAs, and bacteriocin-like inhibitory substances that prevent pathogens. (Tharmaraj and Shah, 2009). Bacteriocins refer to antimicrobial peptides or proteins that are produced by bacteria via ribosomal mechanisms. The aforementioned compounds demonstrate a diverse spectrum of antimicrobial efficacy against pathogenic bacteria, encompassing multiple strains of Staphylococcus, Listeria, Bacillus, Clostridium, and other bacterial species (Dai et al., 2021; Fathizadeh et al., 2022). The significance of bacteriocins synthesised by probiotic bacteria is ascribed to their secure utilisation in diverse domains, including the food industry, pharmaceuticals, veterinary medicine, and human healthcare (Barcenilla et al., 2021; Sharma et al., 2021; Somashekaraiah et al., 2021). The compounds cited in the scholarly articles (Sheoran and Tiwari, 2019; Sheoran and Tiwari, 2020; Chen et al., 2021) exhibit inhibitory effects on a wide range of bacteria. Their mechanism of action involves reducing cell viability, modifying bacterial cell metabolism, and inhibiting toxin production. Additional mechanisms of probiotic action include competitive inhibition on the surface of the intestinal epithelium, wherein the probiotics obstruct the binding sites of the intestinal epithelial surface, as well as a reduction in the interaction between the pathogen and the host. Similarly, the investigation of nutrient competition is also examined as a mechanism underlying probiotic activity. According to the suggestions of the World Health Organization (WHO), Food and Agriculture Organization (FAO), and the European Food Safety Authority (EFSA), in their selection process, probiotic strains must meet both safety and functionality criteria, as well as those related to their technological usefulness. Probiotic characteristics are not associated with the genus or species of a microorganism, but with few and specially selected strains of a particular species (Hill et al., 2014). FAO and WHO have jointly developed guidelines that propose a systematic approach for conducting comprehensive evaluations of probiotics in food products, to provide scientific evidence to support health claims and benefits. The essential criteria for an ideal probiotic are presented by Pandey et al. (2015). The application of the FAO/WHO guidelines on Probiotics has the potential to serve as a universal benchmark for evaluating probiotics in food products, thereby facilitating the validation of health-related assertions.
The guidelines stipulate that the following activities must be carried out:
The identification and categorisation of strains.
• A comprehensive elucidation of the strain(s) about their safety and probiotic attributes.
• Verification of the health benefits observed in human studies.
• Ensuring the accuracy and transparency of efficacy claims and product information throughout the entire duration of the product’s shelf life.
6.1 Probiotics in ulcerative colitisThe colon contains the highest concentration of microorganisms, suggesting treating colon microbiome abnormalities could benefit individuals with ulcerative colitis. Studies have shown potential benefits from various probiotic strains. (Basso et al., 2019). Previous studies have demonstrated that the use of the non-pathogenic strain of E. coli Nissle 1917 (EcN) exhibited similar efficacy and safety characteristics in the maintenance therapy of patients with mild or moderate ulcerative colitis when compared to treatment with salicylates (Basso et al., 2019; Bischoff et al., 2020). The potential therapeutic and prophylactic effects of the probiotic strain EcN against adherent-invasive Escherichia coli (AIEC) infection in zebrafish were investigated. In the zebrafish model, the researchers discovered that EcN effectively reduced AIEC colonisation, tissue damage, and pro-inflammatory responses. Furthermore, EcN reduced AIEC hyperinfection in zebrafish, especially when propionic acid was present. The effectiveness of EcN in combating AIEC infection in a zebrafish model is highlighted in this study. (Nag et al., 2022) The utilisation of various strains of lactic acid bacteria and bifidobacteria as supplementary treatment has been observed to significantly improve the progression of the disease and the sustained absence of symptoms in individuals diagnosed with ulcerative colitis (Basso et al., 2019). A highly regarded probiotic complex is VSL#3, which consists of four strains of Lactobacillus (L. casei, L. acidophilus, L. plantarum and L. delbrueckii subsp. bulgaricus), three strains of Bifidobacterium (B. longum, B. breve, and B. infantis), and one strain of Streptococcus (S. salivarius subsp. termophilus) (Basso et al., 2019). Studies conducted on mouse models have demonstrated that the administration of this probiotic mixture leads to the suppression of NF-B and TNF expression in the TLR4-NF-B signalling pathway. Consequently, the downregulation of pro-inflammatory cytokines and toll-like receptors (TLR) occurs while the upregulation of regulatory cytokines is observed (Jakubczyk et al., 2020; Silva et al., 2020). Previous studies have demonstrated the efficacy of VSL#3 in inducing and sustaining remission in individuals with mild to moderate UC when used as adjuvant therapy or as a standalone treatment (Basso et al., 2019).
In a systematic review and meta-analysis conducted by Derwa et al. (2017), it was found that the VSL#3 probiotic mixture demonstrated potential efficacy in inducing remission among individuals with UC. Furthermore, the study suggested that the use of VSL#3 probiotics may be comparable to 5-5-ASA in terms of preventing disease exacerbations. Under the recommendations put forth by the European Society for Clinical Nutrition and Metabolism (ESPEN), the investigation of probiotics such as VSL#3 and EcN in the treatment of mild to moderate UC is warranted, as they have shown potential for inducing remission in affected patients. According to Bischoff et al. (2020), the use of probiotics is contraindicated in cases of severe ulcerative UC. The use of probiotics as a supplementary treatment may have particular efficacy in the management of patients who experience intolerance to 5-ASA (Miele et al., 2018; Bischoff et al., 2020). Table 2 presents several clinical trial findings regarding the use of probiotics for the treatment of UC.
Table 2 Some clinical trial data of probiotics for treating UC.
7 Prebiotics: nourishing beneficial bacteriaThe term “prebiotics” is a relatively recent concept that is clearly defined as “nondigestible food ingredients that beneficially alter the host by selectively stimulating the growth and/or activity of a specific group of bacteria in the colon, thereby improving the overall health of the host” (Gibson and Roberfroid, 1995). Recently, the International Scientific Association for Probiotics and Prebiotics (ISAPP) convened a panel of experts to reassess the definition of prebiotics. The panel has expanded the definition to encompass a broader understanding, defining it as “a substrate that is selectively utilised by host microorganisms, resulting in a health benefit.” The definition presented by Gibson et al. (2017) expands upon the concept of prebiotics by considering the potential inclusion of non-carbohydrate substances, exploring their relevance to body sites beyond the gastrointestinal tract, and identifying distinct groups beyond those found in food. These substances are typically classified as short-chain carbohydrates that are resistant to digestion yet serve as substrates for the proliferation of probiotic microorganisms within the upper gastrointestinal tract. Cocoa-derived flavanols are compounds that are not classified as carbohydrates but have been proposed as potential prebiotics. According to Tzounis et al. (2011), experimental studies conducted both in vivo and in vitro demonstrate that flavanols can enhance the proliferation of lactic acid bacteria.
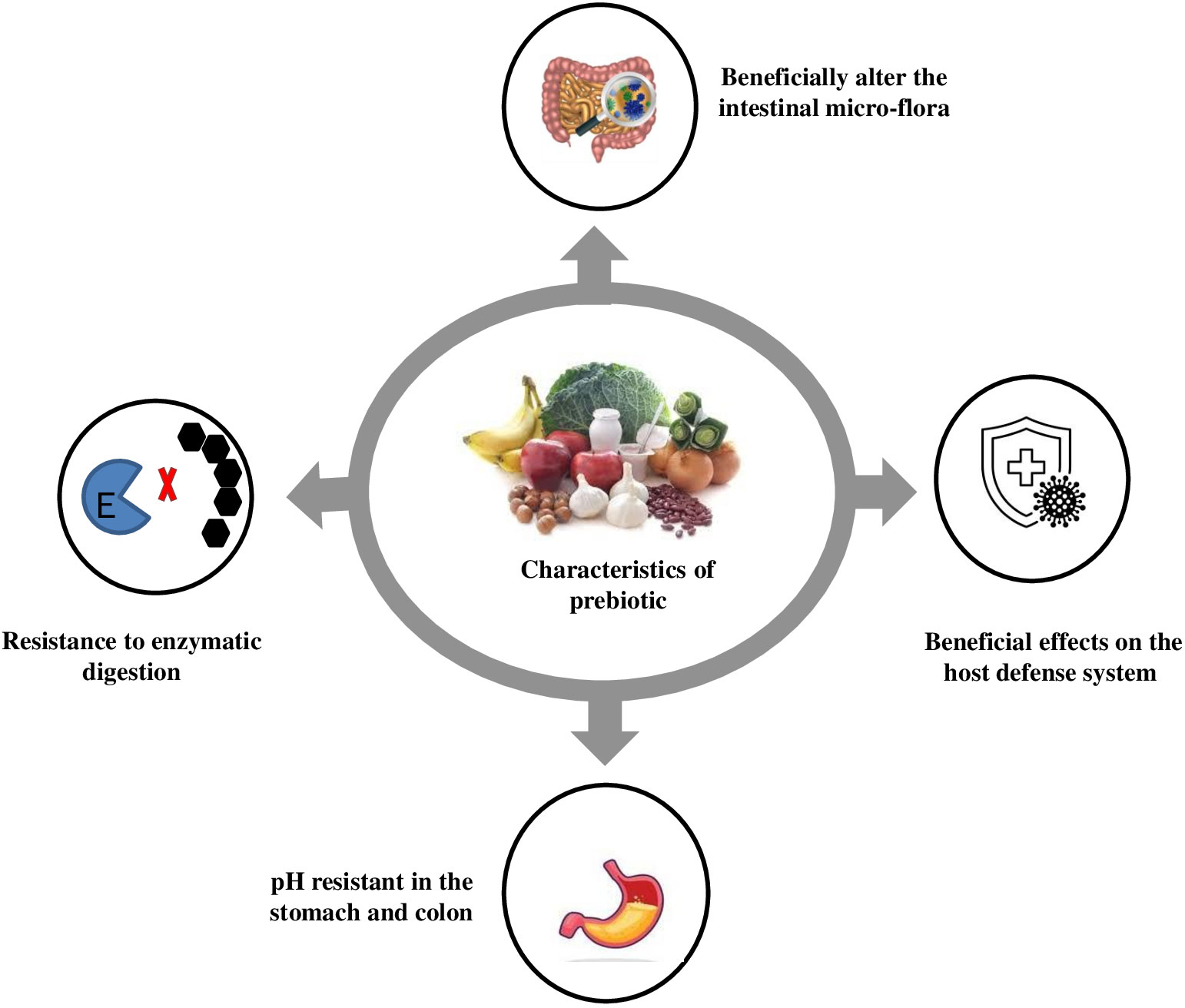
A significant increase in the Bifidobacteria population in faecal samples has been reported due to fructooligosaccharides (FOS) consumption. Prebiotics, consisting of glucose, fructose, galactose and/or xylose, undergo minimal hydrolysis in the intestinal tract and have caloric value due to their resistance to digestion and energy metabolism through fermentation (Roberfroid, 1993). Prebiotics like FOS, isomalto-oligosaccharides (IMO), and xylooligosaccharides (XOS) are studied for their potential benefits on stool volume, constipation relief, and faecal acidity. FOS, like inulin and neosugar, are dietary fibres that improve stool volume and faecal acidity. These prebiotics are easily metabolised by bifidobacteria and other microorganisms like Lactobacillus acidophilus, Bacteroides vulgatus, B. ovatus, B. thetaiotaomicron, B. fragilis, and Enterococcus faecium, E. faecalis (Guarino et al., 2020) An optimal prebiotic substance should possess several key characteristics, as illustrated in Figure 2. IMO can be identified in various fermented food products, including miso, soy sauce, and honey. These compounds are known to be metabolised by bifidobacteria and the Bacteroides groups. IMO facilitates the proliferation of Bifidobacterium and Lactobacillus species, leading to both local and systemic Th1-like immune responses and the regulation of immune function. The presence of positive outcomes has been identified in the clinical trials. XOS are a class of prebiotics that occur naturally in various sources such as fruits, bamboo shoots, vegetables, milk, honey, and others (Aachary and Prapulla, 2010). Previous research has indicated that Bifidobacterium adolescentis can utilise XOS, while, Lactobacillus rhamnosus, L. plantarum and Lactococcus lactis have been found to efficiently metabolise oat -glucooligosaccharides. According to Van Laere et al. (2000), the fermentation process of arabinose-XOS derived from wheat meal by bifidobacteria can be attributed to the existence of xylanolytic enzyme systems such as xylosidase and a limited number of arabinosidases. The presence of a -D-xylosidase derived from Bifidobacterium breve K-110, as well as arabinosidases originating from B. adolescentis DSM20083 (Van Laere et al., 2000) and B. breve (Shin et al., 2000), has been documented in the literature. Zeng et al. (2007) conducted a study on the species B. bifidum, B. adolescentis, and B. infantis, and reported that these species exclusively exhibited arabinosidase and xylosidase activity, while no activity of, glucuronidase, or acetyl xylan esterase and xylanase was observed. Gullon et al. (2008) studied the fermentation process of XOS from rice husks using probiotic bacteria. They found that Bifidobacterium adolescentis CECT 5781 showed significantly greater growth compared to Breve CECT 4839, Bifidobacterium longum CECT 4503 and Infantis CECT 4551 in the presence of XOS. This highlights the importance of industrial development in prebiotics for enhancing food quality and human health.
Figure 2 Characteristics of prebiotic.
A variety of functional foods containing prebiotics have been utilised in the production of biscuits, candies, tabletop sweeteners, frozen yoghurt, and other similar products (Davani-Davari et al., 2019). In Japan, the Foods for Specified Health Uses (FOSHU) programme has incorporated various prebiotics, such as FOS, IMO, XOS, lacto-sucrose, and lactulose oligosaccharides, into specific food products. Additional examples of prebiotic foods include yoghurts, cereals, cakes; cereal bars biscuits high in dietary fibre, powdered beverages, pasta, sauces, bread, infant formula products and various fruit juices (Desai, 2008). Prebiotics are commonly associated with specific types of dietary fibre, such as inulin and FOS. However, they can also be found in various food sources, including cultivated plants and wild plants. Below are several examples of food plants that are abundant in prebiotics; categorised accordingly as cultivated and wild plants.
Cultivated plants
• Bananas: Bananas contain FOS, which is a type of prebiotic that is fermented by beneficial bacteria in the gut. FOS has been shown to advance gut health, decrease inflammation, and improve the immune system. (Sabater-Molina et al., 2009)
• Garlic: Garlic contains inulin, a prebiotic fibre that nourishes gut bacteria. It is also known for its antimicrobial properties. (Davani-Davari et al., 2019)
• Legumes: Legumes, such as beans, lentils, and peas, are excellent sources of resistant starch, a type of prebiotic that is fermented by beneficial bacteria in the gut. Resistant starch has been shown to increase gut health, decrease the risk of chronic diseases, and benefit weight management. (Mirmiran, 2014)
• Oats: Oats are a great source of beta-glucans, a category of soluble fibre that is fermented by beneficial bacteria in the gut. Beta-glucans has been shown to improve gut health, reduce cholesterol levels, and help with weight management. (Sabater-Molina et al., 2009)
• Whole grains: Whole grains, such as brown rice, quinoa, and barley, are excellent sources of resistant starch and other prebiotics. (Sabater-Molina et al., 2009)
• Onion: Like garlic, onions are rich in inulin and can promote the growth of helpful gut bacteria. (Davani-Davari et al., 2019)
• Asparagus: Asparagus is a good source of inulin, a type of soluble fibre that is fermented by beneficial bacteria in the gut. Inulin has been shown to improve gut health, boost immunity, and decrease the risk of chronic disorders. (Sabater-Molina et al., 2009)
• Jerusalem artichoke: Jerusalem artichokes are high in inulin content, making them an excellent prebiotic food. (Sabater-Molina et al., 2009)
• Chicory Root: Chicory root is often used as a source of inulin in supplements, which is proven to increase the growth of Bifidobacterium. It can be consumed raw or roasted (Davani-Davari et al., 2019).
Wild Plants:
• Taraxacum officinale (Dandelion greens): A very common plant, dandelion grows wild almost everywhere. Dandelion is a native of Europe. In India, it is found in the Himalayas. Nutritionally, the dandelion has remarkable value. Dandelion greens are wild plant that contains inulin and other prebiotic fibres, along with various nutrients (Wirngo et al., 2016).
• Arctium lappa L (Burdock Root): Burdock root is a wild plant that contains inulin and has been traditionally used as a medicinal food with prebiotic properties. This species is native to the temperate regions of the Old World, from Scandinavia to the Mediterranean, and from the British Isles through Russia, and the Middle East to India, China, Taiwan and Japan. (Moro and Clerici, 2021).
• Cichorium intybus L (Chicory Greens): Wild chicory greens are rich in inulin and can be consumed in salads or cooked as a side dish. The Chicory crop is cultivated in a few States, mostly Uttar Pradesh, and Gujarat. These two states account for 97% of the total production of Chicory in India (Nwafor et al., 2017).
• Musa paradisiaca (Plantain): Plantain leaves are a common wild plant that contains prebiotic fibres, among other beneficial compounds. Plantain fruit is widely consumed in Nigeria, Africa and some other parts of the world (Ukwah et al., 2014).
• Urtica Dioica (Nettles): Nettles are known for their numerous health benefits and can provide prebiotic effects due to their fibre content. It is most common in Europe, North America, North Africa, and parts of Asia (Behzad et al., 2018).
These are just a few examples, and there are many other cultivated and wild plants that can offer prebiotic benefits. Combining a type of these prebiotic-rich foods into your diet can aid in promoting a healthy gut microbiome (Crittenden and Playne, 2008; Davani-Davari et al., 2019). For a product (food or supplement) to be believed to be a prebiotic, it must meet the below-mentioned conditions (Gibson et al., 2017).
Prebiotic enhance the proliferation and metabolic function of selected bacterial strains that exhibit beneficial impacts on overall well-being in the following ways.
• Lower the pH of the substances presents in the intestines.
• To exhibit resistance to hydrolysis and the effects of gastrointestinal enzymes.
• To avoid being absorbed in the upper gastrointestinal tract.
• To maintain a suitable environment for one or more beneficial microorganisms within the colon.
• To maintain stability throughout the food processing procedure,
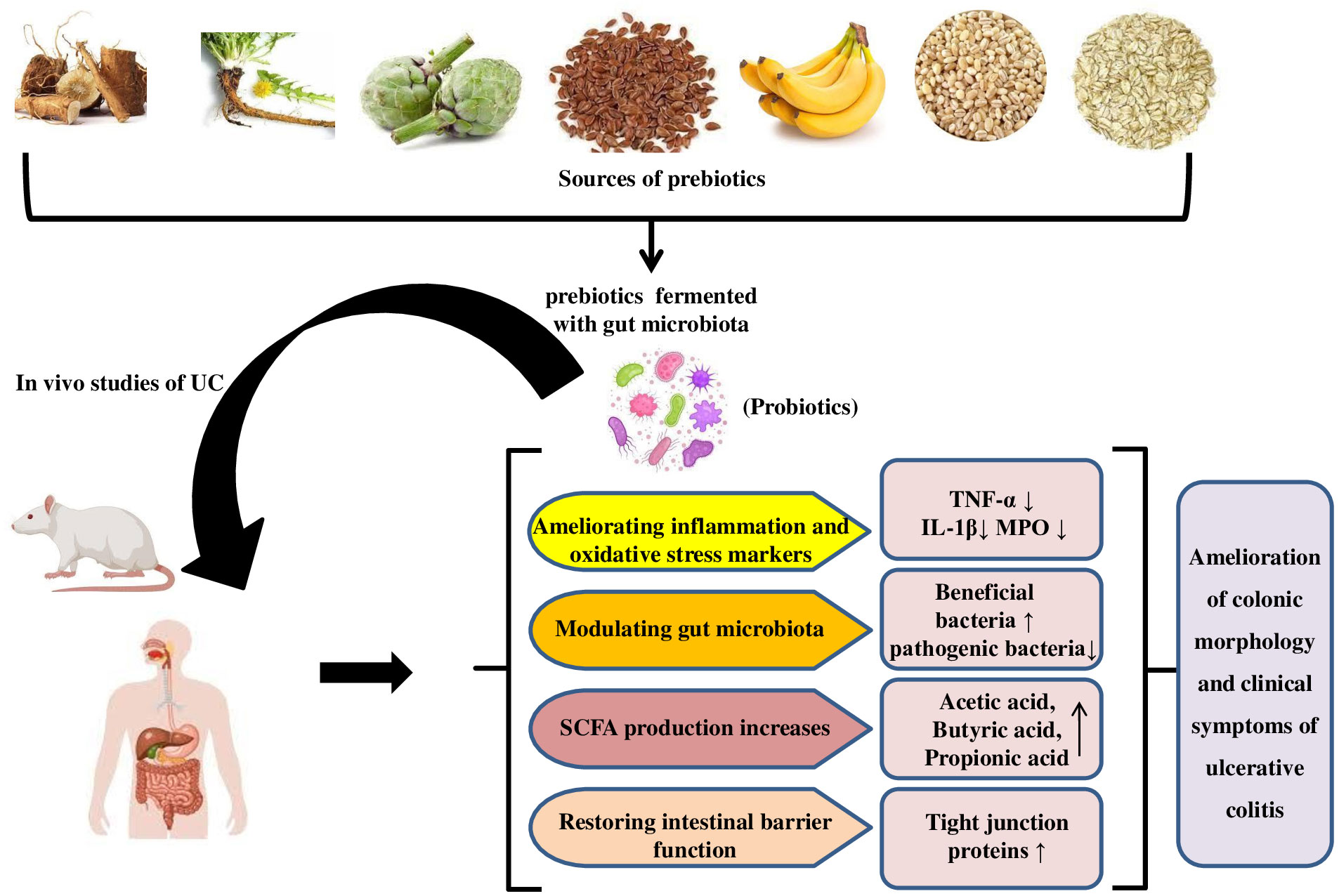
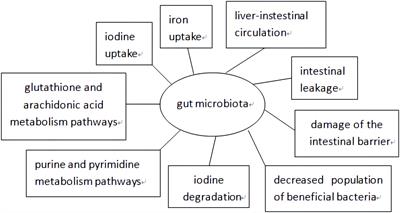
7.1 Prebiotics in UCPrebiotics, mostly fermentable carbohydrates, promote local or systemic health (Pandey et al., 2015; Akram et al., 2019). Prebiotics can alter the intestinal microbiota, improve the intestinal barrier, and promote the growth of beneficial microbes in the digestive tract, which produce host-beneficial metabolites. (Aljuraiban et al., 2023) Like probiotics, clinical trials on prebiotics in specific diseases are difficult to prove. Thus, prebiotic data in UC patients is carefully regulated. Prebiotics may help treat UC by supplementing fermentable carbohydrate-containing fibre fractions. Promoting specific bacteria and/or their metabolites achieves this (Pandey et al., 2015; Rasmussen and Hamaker, 2017). Prebiotics may help maintain remission or low clinical disease activity. Prebiotics used in UC studies are oligosaccharides and inulin (Rasmussen and Hamaker, 2017). The mechanism for the ameliorative effect of prebiotics in UC studies is illustrated in Figure 3. Prebiotics encourage the growth of beneficial microorganisms, which compete with harmful species and produce beneficial fermentation substances like SCFAs, which have immunomodulatory properties and influence toll-like receptor-4 signalling and pro-inflammatory cytokines. (Van der Beek et al., 2017)
Figure 3 Mechanism for ameliorative effect of prebiotics in UC studies.
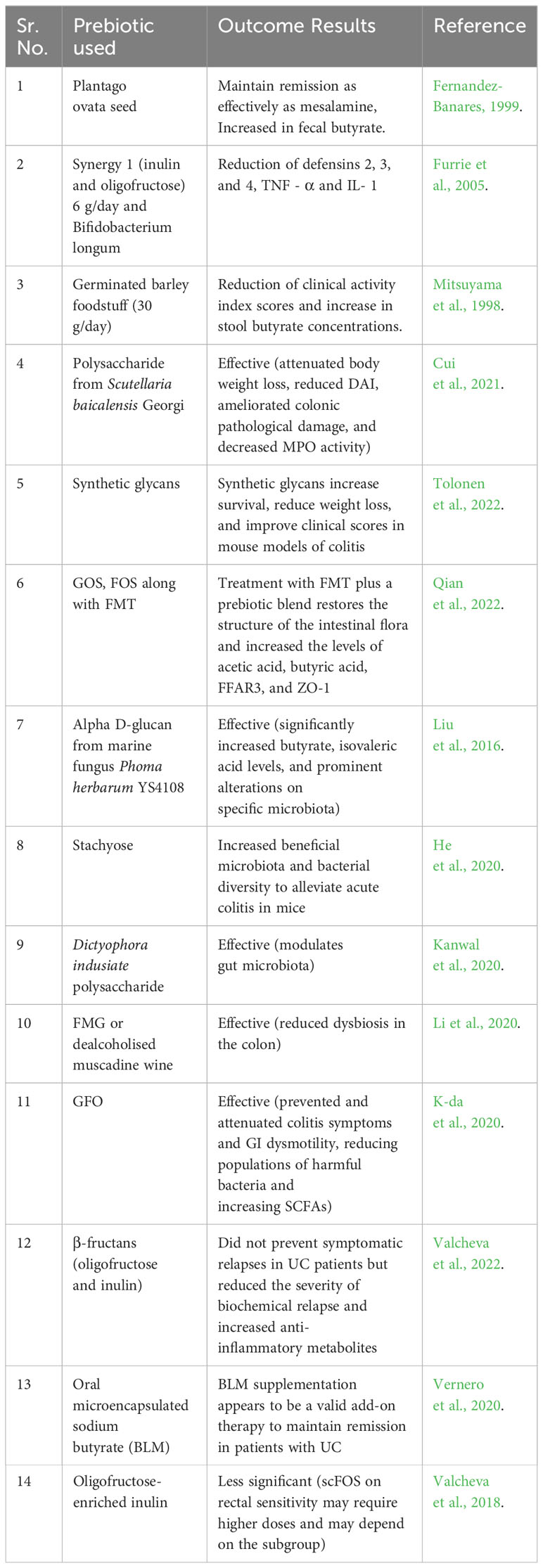
Casellas et al. (2007) studied the effects of mesalazine treatment, oligofructose-enriched inulin, and placebo on patients with mild to moderate UC. Oral oligofructose-enriched inulin was well-received and reduced faecal calprotectin levels. Faecal calprotectin has been employed as a reliable and quantifiable indicator of intestinal inflammation, with a significant correlation observed between its levels and the assessment of disease activity in UC, as determined through histologic and endoscopic methods (Konikoff and Denson, 2006).In Japan, germinated barley food (GBF) has been explored as a therapeutic intervention for UC. GBF, a dietary fibre and protein-rich in glutamine, has been shown to reduce clinical activity in individuals with UC and is an effective treatment option for maintaining remission. The safety profile of the treatment is noteworthy, as the study conducted by Hanai et al. (2004) found no incidence of side effects in the study group associated with the use of GBF. Nevertheless, further clinical trials are required to provide additional confirmation regarding the efficacy of dietary fibre as a prebiotic in the management of UC. Prebiotics has been extensively utilised in the management and treatment of UC. Table 3 presents a comprehensive compilation of various studies that have examined the advantageous effects of prebiotics in the management of UC.
Table 3 Studies of prebiotics in the management of UC.
8 SynbioticsGibson’s proposition of prebiotics was accompanied by a rationale for the potential advancements that could be achieved through the combination of prebiotics with probiotics, leading to the establishment of what he referred to as Synbiotics (De Vrese and Schrezenmeir, 2008). The term “synbiotics” pertains to the amalgamation of prebiotics and probiotics to improve the well-being of humans or animals (Markowiak and Śliżewska, 2017). According to research conducted by Perrin et al. (2001) and Sharma and Shukla (2016), the probiotic bacteria found in synbiotic food products make selective use of prebiotics as a substrate for their growth. A group of specialists from the International Scientific Association for Probiotics and Prebiotics got together and rethought the concept of synbiotics. Synbiotic treatment aims to improve the endurance and metabolic function of beneficial probiotic strains in the gut microbiota. Common combinations include lactobacilli and bifidobacteria with oligosaccharides, inulin, or fibres as prebiotics. This approach reduces systemic inflammation by increasing the population of bacteria producing SCFAs and providing substrates for fermentation (Pandey et al., 2015).
According to their classification, synbiotics can be categorised into two distinct classes: complementary and synergistic. A complementary synbiotic is comprised of a probiotic and a prebiotic, which collectively provide one or more health benefits without requiring interdependent functions. According to Swanson et al. (2020), a synergistic synbiotic is composed of a substrate that is specifically utilised by microorganisms that are co-administered. These guidelines are expected to be efficacious in establishing expectations regarding the comprehension of the interplay between pre- and probiotics as well as the advancement of synbiotic products for the promotion of health and therapeutic interventions. Numerous reports suggest that the consumption of synbiotic foods has a beneficial impact on the health and nutritional status of the host. The study conducted by Yang et al. (2005) revealed that the administration of synbiotics had a dual effect on the faecal sample. Firstly, it was observed that synbiotics increased the abundance of probiotic bacteria, specifically Lactobacillus and Bifidobacterium, while simultaneously reducing the presence of coliform bacteria. Additionally, the test group exhibited an improvement in the levels of various digestive enzymes, including lactase, sucrase, lipase and isomaltase. Recently, there has been a report indicating that the consumption of synbiotics has significantly decreased various cardiovascular risk factors, the prevalence of metabolic syndrome, and markers of insulin resistance among elderly individuals (Cicero et al., 2021). The ability of bifidobacteria to metabolise prebiotics is dependent on the species, which is a valuable characteristic for modulating the gut microbiota through the use of specialised prebiotics (Bielecka et al., 2002; Biedrzycka and Bielecka, 2004). The β-fructofuranosidase enzyme derived from Bifidobacterium adolescentis G1 exhibits a preference for fructooligomers over inulin as its substrate. This preference is also observed in B. bifidum. In contrast, it has been observed that B. longum and B.animalis possess the ability to hydrolyze a diverse array of FOS and XOS, including those derived from inulin (Bruno et al., 2002). According to a study conducted by Bruno et al. (2002), food products contain the greatest concentration of viable bifidobacteria. Likewise, the efficacy of B. longum supplemented with FOS is greater in curd. According to Martinez-Villaluenga and Gomez (2007), the probiotic B. lactis possesses the enzymes β-glucosidase and β -fructofuranosidase, which enable it to metabolise oligosaccharides present in fermented milk. This metabolic activity promotes the growth and metabolism of the probiotic organism. The therapeutic potentials and health benefits of different probiotics, prebiotics, and synbiotics are presented in Table 4.
Table 4 Therapeutic potential and health benefits of probiotics, prebiotics and synbiotics.
8.1 Synbiotics in ulcerative colitisSynbiotics are products that combine probiotics and prebiotics, resulting in a synergistic interaction. This concept was introduced to address challenges in probiotic survival, especially during transit through the upper gastrointestinal tract. The use of a synbiotic enhances probiotic colonisation efficacy and facilitates the proliferation of probiotic strains (Pandey et al., 2015).
There is a limited body of research examining the impact of a synbiotic supplement on individuals diagnosed with UC. Table 5 presents a compilation of the studies that have been cited most frequently and illustrated in Figure 4. Wong et al. (2022) investigated the impact of prebiotic mixtures, probiotic mixtures, and synbiotics on colitis in a murine model. The findings of the study indicated that the administration of synbiotic treatment had a protective effect on the structure of the colon, as evidenced by the preservation of its integrity. Furthermore, there was an observed increase in the expression of occludin, a protein involved in maintaining the tight junctions between cells, which is indicative of improved barrier function. Additionally, the treatment was found to be effective in reducing the infiltration of cells into the colon and resulted in alterations to the gut microbiome, enhancements in colonic integrity, and the suppression of markers associated with inflammation. Although the existing studies have yielded promising results thus far, it is important to note that the methodologies employed often exhibit inconsistencies, lack proper description, and/or suffer from inadequate study design. Additionally, it is worth mentioning that the majority of cases have been characterised by a notably limited number of registered patients.
Table 5 Summary of the most relevant studies involving synbiotics treatments in UC.
Figure 4 Use of synbiotics for ulcerative colitis treatment.
9 Safety and considerations in ulcerative colitis treatmentWhen it comes to treating ulcerative colitis, ensuring safety and considering various factors are of paramount importance. Here are some key safety considerations to keep in mind:
9.1 Medical supervisionUlcerative colitis treatment should always be conducted under the guidance and supervision of a qualified healthcare professional. They will assess the severity of the condition, consider individual patient factors, and prescribe appropriate medications or therapies (Kerner et al., 2014).
9.2 Monitoring and follow-upRegular monitoring is crucial to evaluating the effectiveness of the treatment and assessing any potential side effects or complications. Patients should attend follow-up appointments as scheduled and communicate any changes in symptoms or concerns to their healthcare provider (Click and Regueiro, 2019).
9.3 Medication safetyPatients need to follow the prescribed medication regimen diligently. They should be aware of potential side effects and know when to seek medical attention. Certain medications used in ulcerative colitis treatment, such as immunosuppressants or biologics, may require additional precautions and monitoring due to their impact on the immune system (Click and Regueiro, 2019).
9.4 Individualised approachEach patient with ulcerative colitis is exceptional, and management plans should be designed to meet their special needs. Factors such as age, disease severity, comorbidities, and medication tolerance should be taken into consideration when developing a personalised treatment strategy (Kerner et al., 2014).
9.5 Lifestyle modificationsIn addition to medication, lifestyle changes can play a major role in managing ulcerative colitis. These may include dietary changes, stress management techniques, regular exercise, and getting sufficient rest. Patients should work with healthcare professionals, such as dietitians and psychologists, to make appropriate lifestyle adjustments (Click and Regueiro, 2019).
9.6 Risk-benefit assessmentEvery treatment decision involves a careful evaluation of the potential risks and benefits. Patients and healthcare providers should discuss the expected outcomes, potential side effects, and long-term implications of various treatment options. This shared decision-making process ensures that the chosen treatment aligns with the patient’s goals and preferences (Kerner et al., 2014).
9.7 Complementary and alternative therapiesIf considering complementary or alternative therapies, patients should consult with their healthcare provider to ensure safety and assess potential interactions with conventional treatments. It is important to be cautious of unproven or unsupported therapies that may promise a cure without scientific evidence (Click and Regueiro, 2019).
9.8 Patient education and supportPatient education about their condition, treatment options, and self-care is essential. Ulcerative colitis patients can benefit from educational resources and support groups. In conclusion, ulcerative colitis treatment must prioritise safety and individual factors. Patients can manage their condition while minimising risks and maximising treatment benefits with medical supervision, regular monitoring, personalised approaches, and informed decision-making (Kerner et al., 2014).
10 Future perspectives and researchUC significantly impacts individuals’ health and quality of life, with treatment options including aminosalicylates, corticosteroids, immunomodulators, biological therapies, and surgical interventions. However, some patients have not responded well to these treatments, leading to prolonged suffering and reduced quality of life. Alternative therapies like experimental drugs are considered, but their effectiveness remains uncertain and comes with risks and complications. As we gain more understanding of the pathophysiology of UC and its relationship with the microbiome, there will be a rise in research trials to determine the efficacy of emerging treatments. Scholars are currently investigating “next-generation” probiotics, such as Clostridium clusters IV, XIVa, and XVIII, Bacteroides uniformis, Bacteroides fragilis, Akkermansia muciniphila, Eubacterium hallii, and Faecalibacterium prausnitzii as potential alternatives.
Collaborative engagement between patients and healthcare providers is crucial for determining the most suitable treatment approach. Emerging treatments like prebiotics, probiotics, and synbiotics have gained attention for their potential therapeutic benefits in improving gut h
留言 (0)