
Remember me







where P is the 17O concentration (%); TE is the effective TE; R2(17O) is the transverse relaxivity (1/s%); S indicates signals; S0 indicates baseline signals; and 0.037 is the natural abundance of 17O (%).
Moreover, note that R2(17O) (1/s%) varies with temperature, pH, and solute concentration, among others.50,52
Spin echo or FSE is an essential sequence in clinical MRI and can be combined with various imaging methods, such as 2D, 3D, and fluid-attenuated inversion recovery27 with inversion pulses to suppress CSF signals. Therefore, SE or FSE is easy to apply in basic and clinical research; however, if a longer echo time is used to obtain a higher T2 contrast for water imaging, the SNR decreases, making the evaluation of parenchymal organs, such as the brain parenchyma, difficult (Fig. 2A). Echo planar imaging can also be used to achieve a higher temporal resolution.59,60
Another candidate sequence in the T2WI category for detecting 17O-induced proton signal intensity changes is steady-state free precession (SSFP).23,24 In this sequence, a steady-state condition is achieved by applying a sequence of radiofrequency pulses and gradients, which allows for high SNR and fast imaging (Fig. 2B). Steady-state free precession has a T1/T2 contrast, is often used for cardiac imaging, and can provide information on myocardial perfusion. It has several advantages such as a higher SNR and higher spatial or temporal resolution for dynamic imaging. However, banding artifacts can become severe with a longer echo or TR to achieve higher contrast.23 Absolute quantification has been achieved with phantom measurements and signal simulations; however, voxel-wise calculation is only possible after determining the T1 and T2 values of the voxel.24
Another sequence used to indirectly detect 17O-labeled water is T1rho, which measures the T1 relaxation times of water molecules in the presence of a spin-lock pulse.31,61–66 This sequence is sensitive to changes in tissue properties, such as pH and macromolecular content, and is often used in imaging cartilage and other musculoskeletal tissues. The basic idea behind T1rho MRI is that, when a sample is exposed to a magnetic field, the magnetic moments of 17O and adjacent protons precess around the field axis at different rates due to differences in their chemical shifts. This leads to JJ vicinal coupling between 17O and adjacent protons, which in turn affects the T1rho relaxation time of the protons. By detecting the T1rho relaxation time of protons, the presence of 17O can be indirectly inferred. To perform T1rho imaging, a series of radiofrequency pulses with different flip angles and time delays is applied to the sample to measure the T1rho relaxation time of the protons. Then, a spin-lock pulse is applied to the sample to saturate the longitudinal magnetization and induce T1rho relaxation. After the application of the spin-lock pulse, a readout pulse is applied to measure the proton signals. T1rho imaging has several advantages over other indirect methods. For example, this technique is less sensitive to patient motion and susceptibility artifacts. Furthermore, it can be used to map the distribution of T1rho relaxation times, allowing for more accurate localization of 17O in tissues. A disadvantage of T1rho imaging is that it is sensitive to B1 field inhomogeneities, which can lead to errors in the measured T1rho relaxation time. Furthermore, it can be affected by the presence of other macromolecules in the tissue, which can cause T1rho relaxation effects unrelated to 17O.
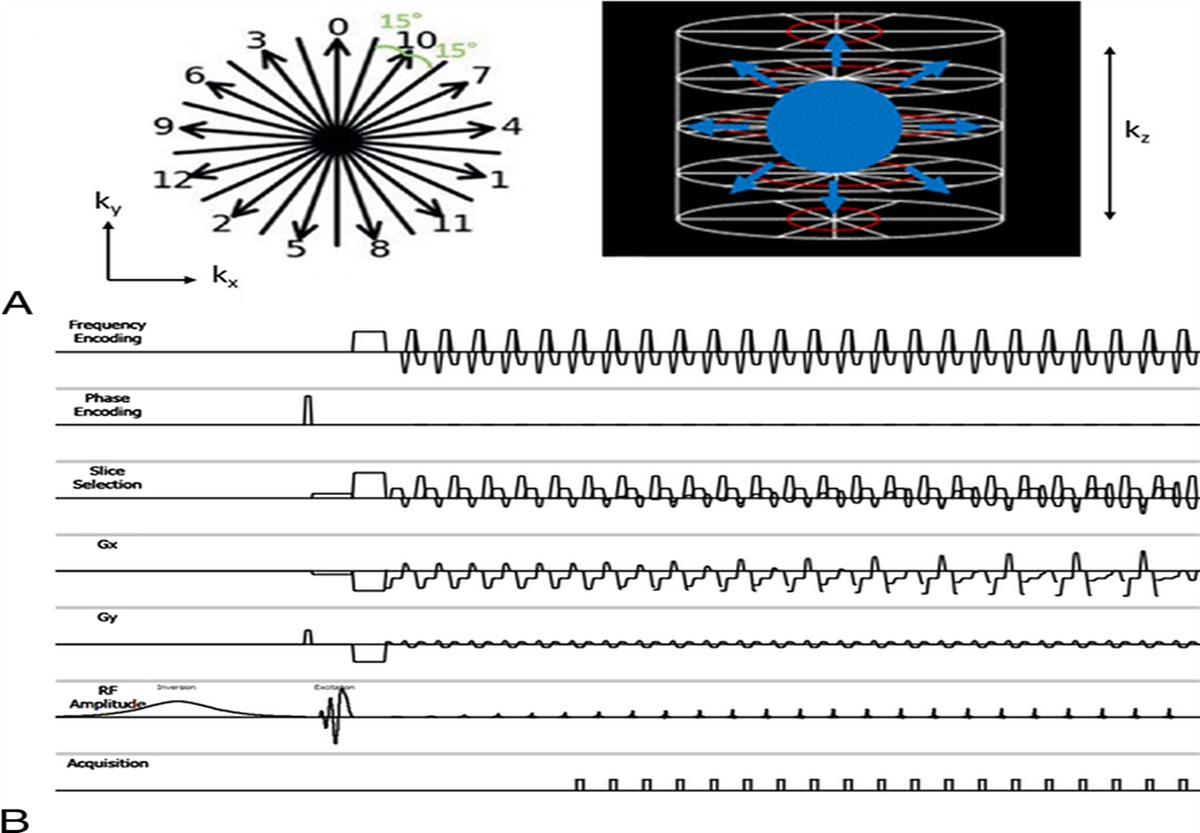
JJ vicinal coupling proton exchange (JJVCPE) imaging is a technique that uses the JJ vicinal coupling between 17O and adjacent protons in water molecules to indirectly image 17O.36,67,68 This technique can deduce the location of 17O from adjacent proton signals even when the signal from 17O is insufficient for 17O-MRI (direct method). In JJVCPE imaging, a chemical shift–selective excitation pulse is used to selectively excite the signal from protons adjacent to the 17O atom. After this excitation, a series of phase-encoding gradients is applied to encode the spatial location of the water molecule in each voxel. Subsequently, a fast SE readout is used to detect proton signals. The key idea behind JJVCPE imaging is that the signal from adjacent protons is influenced by the JJ vicinal coupling between 17O and the protons, which in turn is affected by the rate of water molecule proton exchange. By analyzing the signal from the protons, the location of 17O in each voxel can be indirectly inferred, and a 17O image can be conducted. The JJVCPE imaging has several advantages over other indirect methods for detecting 17O-labeled water. For example, this technique is less sensitive to patient motion and susceptibility artifacts. Furthermore, it can be used to perform voxel-wise mapping of the 17O signal, enabling more accurate localization of 17O in tissues. However, a disadvantage of JJVCPE imaging is that it requires long acquisition times, which can be a limitation in clinical applications. Moreover, this technique is sensitive to off-resonance effects that can lead to artifacts in the resulting images.
The 17O-decoupled method can also be used to detect 17O by proton MRI. By irradiating protons with continuous-wave radiofrequency, the coupling effect between 17O and proton nuclei is eliminated, and a prolonged T2 of the water proton is observed. By subtracting the images obtained with decoupling from those obtained without decoupling, the amount of 17O can be measured; however, this decoupling method requires additional specific hardware and some special knowledge, similar to 17O-MRI (direct method).55,60,69,70 A high specific absorption rate is another problem.
Deuterium oxide, commonly referred to as heavy water (D2O), is another potential water tracer that can be used in MRI. Heavy water contains deuterium, a stable hydrogen isotope, which is twice as heavy as the more common hydrogen isotope. Magnetic resonance imaging of heavy water can be achieved through both direct and indirect methods, such as 17O-labeled water. The direct method captures signals at the resonance frequency of 2H, which offers good specificity to deuterium but suffers from low sensitivity, similar to the direct method for 17O. In contrast, in 1H-MRI, proton signals are used, and the proton signals decrease by the H2O-D2O replacement effect,71–74 allowing for higher sensitivity than that of the direct method. Recently, this high sensitivity has been exploited in 1H-magnetic resonance spectroscopic imaging (1H-MRSI) to map metabolites of deuterium-labeled compounds.75,76 Regarding safety, its isotope effect may cause biological toxicity. Animal experiments have suggested significant adverse effects, particularly when administered in large quantities (the toxicity threshold being approximately 30%–40% concentration),77 making its application to humans, particularly in high-concentration formulations, challenging. Generally, the isotope effect increases with a higher mass ratio than the original atom, and because protons are involved in numerous enzymatic reactions within the human body, the biological impact of heavy water is thought to be greater than that of 17O-labeled water. Currently, we have not found any GMP-grade formulations of heavy water suitable for human administration. For the preclinical grade product, the cost is approximately $10/mL,74 making it inexpensive compared with 17O-labeled water.
Oxygen-15 (15O)–labeled water is used as a direct water tracer in positron emission tomography (PET), and 15O-labeled water PET has become an established technique for evaluating cerebral and myocardial blood flow.78–86 However, because of the short half-life of 15O (only 122 seconds), it is not feasible for long-term water dynamics tracking. Radiation exposure and the limited spatial resolution inherent in PET scanners also pose limitations. In contrast, 17O-labeled water can be used with MRI, which offers high spatial resolution without radiation exposure. The synthesis of 15O-labeled water requires a cyclotron facility, and the precursor materials (ie, deuterium gas, nitrogen gas, and hydrogen gas) are relatively inexpensive as precursor materials for PET agents; however, the cost depends on the operating expenses of the cyclotron facility.
In MRI using solute tracers (Gd contrast agents), MR angiography (MRA), MR venography (MRV), and perfusion imaging (dynamic susceptibility contrast [DSC] and dynamic contrast-enhanced) provide information about the vascular structure and dynamic behavior of the solute tracer. However, note that the biophysical behavior of the solute (Gd chelates) differs from that of the solvent (water molecules), and therefore, in certain organs (eg, brain tissue with a blood-brain barrier), the dynamics of water may not be directly reflected by these solute tracers.
In addition, many other nontracer MRI techniques allow for the evaluation of water dynamics. In static imaging, high-quality multiparametric quantitative MRI provides various quantitative values, such as longitudinal relaxation rate (R1), apparent relaxation rate (R2*), proton density (PD), and magnetization transfer saturation, which are sensitive to iron, myelin, and water content in tissue microstructure.2,87,88 However, these parameters do not directly yield information about water dynamics. Dynamic imaging includes several techniques, such as nonenhanced MRA/MRV and diffusion-weighted imaging.89–93 The application range of MRA/MRV through the arteries and veins using time-of-flight or phase-contrast (PC) techniques is limited to large vessels and cannot be applied to slow water dynamics in tissues.3 Diffusion-weighted imaging only provides statistical probabilities of water motion within a narrow time range (milliseconds). Magnetization spin labeling techniques allow the use of endogenous water in the body, including arterial spin labeling (ASL),94 time-spatial labeling inversion pulse,95 and cine MRI with selective labeling of endogenous water in the body. These techniques, similar to 17O-labeled water, can directly provide information on water dynamics. However, because of the short lifespan of tracers (a few seconds) dependent on T1 relaxation, they pose critical challenges for long-term tracking of water dynamics.
17O-labeled water can be used as a freely diffusible tracer to measure blood flow using MRI, similar to 15O-PET. When 17O-labeled water is injected into the bloodstream, it reaches the capillaries, then diffuses out of the vasculature and replaces the water in brain tissues.23–25,27,41,57,96–99 This shortens the T2 values that can be imaged by MRI. Infusion of 17O-labeled water via the carotid artery in a rat showed a signal decrease in T2WI in the brain parenchyma corresponding to the perfusion area of the ipsilateral internal carotid artery (Fig. 3). Theoretically, the blood can be calculated by measuring the signal intensity of the tissue over time. Kwong et al59 reported cerebral blood flow (CBF) measurements using an echo planar imaging sequence after intra-arterial injection of 17O-labeled water (45%) via the external carotid artery. Cerebral blood flow was quantified using a simple compartment model.
 FIGURE 3:
FIGURE 3: Dynamic 17O water-enhanced MRI with intra-arterial infusion in preclinical studies. The 17O concentration map at the unilateral carotid arterial infusion model rat using 17O-labeled saline (20 mol%). The continuous T2WI was acquired on a preclinical proton 7 T MRI using 2D fast spin echo sequence (TR/TE, 3000/100.4 milliseconds; echo train length, 32; thickness, 1.5 mm; in-plane resolution, 0.3 × 0.3 mm; time resolution, 12 seconds). The 17O concentration was estimated from the calculation formula indirect method. The figure indicates the time elapsed after injection completion.
CBF=100λτ+C
where λ is the brain-blood partition coefficient of water, τ is the tracer mean transit time, and C is a constant.
The measurement of arterial concentration (arterial input function) is required for more accurate quantification of CBF. Arai et al96 used the FSE sequence to measure signal changes in the brain after intravenous injection of 17O-labeled water, and CBF was quantified with arterial input function measurements using NMR spectroscopy. They also reported CBF changes during hypercapnia. Indirect 17O-MRI can also visualize pathological conditions, such as cerebral ischemia57,97,100,101 and tumor blood flow/oxygen metabolism.58,102–105
The T1rho technique can be used to quantify CBF. Tailor et al64 reported that CBF could be quantified after intra-arterial injection of 17O-labeled water (29%) via the external carotid artery in the rat brain. They used the simple first-order model by Kety106:
Cbτ=Q∫0τCateQ/λr−tdt
where Cb and Ca are 17O concentrations in excess of the natural abundance in brain tissue and arterial blood, respectively, and Q is the CBF. The same group also reported the tumor blood flow in mice using the same method.65
According to these studies, CBF measurements using 17O-labeled water have several advantages. Theoretically, it would be more accurate in measuring blood flow in tissues because 17O-labeled water is a diffusible tracer, similar to 15O water PET, compared with MR perfusion (DSC), which uses solute tracers. In addition, no radiation exposure or high spatial resolution is achieved, and longer tracing is possible. However, the current cost of 17O-labeled water is expensive, limiting its clinical application compared with other CT or MR methods for CBF measurements, such as CT perfusion and MR perfusion (ie, DSC, dynamic contrast-enhanced, and ASL). Furthermore, no studies have compared the quantitative values of CBF obtained through 17O-labeled water imaging with these existing methods. This is likely because some established and cost-effective methods can measure CBF with sufficient accuracy for clinical use without the need for 17O-labeled water.
We developed an MRI method for quantifying CBF through the intravenous administration of 17O-labeled water using an indirect method.23,27 Other groups have also validated the feasibility of imaging CBF using a 17O indirect method on 3 T MRI.25 In our clinical study involving healthy subjects, intravenous administration of 20 mol% 17O-labeled water resulted in significant 17O concentration changes in the brain parenchyma, subarachnoid space, and lateral ventricles of the brain surface (Fig. 4). These results suggest that intravenous administration of 17O-labeled water can be used for CBF analysis and CSF aqueous dynamics analysis.
 FIGURE 4:
FIGURE 4: First-in-human: water dynamics in the brain with intravenous injection of 17O-labeled water. The 17O concentration map obtained by (A) continuous T2-weihgted FIESTA (fast imaging employing steady-state acquisition) and (B) 3D-FLAIR images on proton 3 T MRI using intravenous (IV) injection of 17O-labeled water (10 mol% 1 mL/kg or 20 mol% 1 mL/kg) in normal volunteers. Time-concentration curves were obtained for the cerebral cortex, ventricle, and subarachnoid space (SAS). Placebo refers to the same amount of physiological saline.
CSF and Glymphatic SystemThe CSF space surrounds the brain and spinal cord, and is filled with CSF, which helps protect these organs from injury and facilitates the transport of nutrients and waste products (Fig. 5).107–109 By providing a constant supply of nutrients and removing waste products, CSF helps regulate the chemical and ionic composition of the brain and spinal cord, maintaining an optimal environment for neural activity. In addition, CSF also contributes to regulating the intracranial pressure. It interacts with the vascular and lymphatic systems and is involved in immune responses in the central nervous system (CNS).
 FIGURE 5: Schematic overview of water dynamics in the CNS and MRI techniques. CNS hydrodynamics include blood flow (arterial, venous, and capillary), CSF, and interstitial fluid (ISF), and each has a different temporal and spatial scale, requiring specific MR sequencing techniques tailored to their characteristics. The pathways shown in figures (A, perivascular space–ISF; B, ISF–perivenular space; C, capillary-ISF; D, ISF-CSF; E, convective flow in ISF) illustrate the glymphatic system, defined as an astrocyte-mediated fluid exchange of CSF and ISF within the brain. The endothelium of astrocytes expresses the water channel aquaporin (AQP)-4, which is thought to be involved in perivascular water influx. Although AQP-4 is a water channel with selective properties, its convective transport has been debated from a physiological standpoint, making it the most controversial aspect of the glymphatic system. DTI-ALPS, diffusion tensor image analysis along the perivascular space.89 Time-SLIP, time-spatial labeling inversion pulse.
FIGURE 5: Schematic overview of water dynamics in the CNS and MRI techniques. CNS hydrodynamics include blood flow (arterial, venous, and capillary), CSF, and interstitial fluid (ISF), and each has a different temporal and spatial scale, requiring specific MR sequencing techniques tailored to their characteristics. The pathways shown in figures (A, perivascular space–ISF; B, ISF–perivenular space; C, capillary-ISF; D, ISF-CSF; E, convective flow in ISF) illustrate the glymphatic system, defined as an astrocyte-mediated fluid exchange of CSF and ISF within the brain. The endothelium of astrocytes expresses the water channel aquaporin (AQP)-4, which is thought to be involved in perivascular water influx. Although AQP-4 is a water channel with selective properties, its convective transport has been debated from a physiological standpoint, making it the most controversial aspect of the glymphatic system. DTI-ALPS, diffusion tensor image analysis along the perivascular space.89 Time-SLIP, time-spatial labeling inversion pulse.Recently, the glymphatic system has gained much attention in the field of human water dynamics.110–113 This system has been proposed as a waste clearance system in the brain, responsible for removing toxins and other waste products, including proteins and other metabolites, which can accumulate in the brain over time and contribute to neurodegenerative diseases and neurological disorders. For example, neurofibrillary tangles and a specific protein called abnormal amyloid-β protein accumulate in the brain in Alzheimer disease (AD). It has been reported that water dynamics related to the aquaporin (AQP)-4 channel (which facilitates water transport) play an important role in eliminating amyloid-β proteins.112,114–116 Thus, CSF has many functions in maintaining CNS homeostasis; however, the sites of its production and absorption, its dynamics in the subarachnoid space and ventricles, and its circulation, including communication between CSF and the brain interstitial fluid (as suggested by the glymphatic hypothesis),111 are not fully understood. Although macroscale water dynamics, such as blood flow, is well understood in many organs and their measurements are widely applied clinically, the physiology and assessment methods of neurofluids are not yet fully understood and established.
To evaluate CSF dynamics or the glymphatic system using 17O-labeled water, various administration routes can be considered. Intravenously administered 17O-labeled water is distributed in the brain parenchyma, and CBF measurements can be performed as previously mentioned. In addition to the measurement of the brain parenchyma, signal changes in the CSF space can be achieved using several methods, including FSE, JJVCPE, and SSFP. In the clinical trial mentioned earlier, the temporal changes in 17O concentration differed between the subarachnoid space on the brain surface and within the lateral ventricles, with the change in 17O concentration being more gradual within the lateral ventricles (Fig. 4). This early distribution of water tracers into the subarachnoid space has also been confirmed in human studies targeting blood-to-CSF water transport using ultra-long TE ASL, although it requires a long scan time.94 These findings suggest that the CSF leaks from the choroid plexus (classic site of CSF production) vessels traveling in the subarachnoid space and the brain surface.107 With aging, an increase in the amount of connective tissue between the brain parenchyma and vascular endothelial cells has been reported, leading to a physiological reduction in CSF.117 Decreased CSF production also results from altered clearance of brain waste products associated with the progression of dementia, including AD.118 Although we have only conducted MRI studies of intravenous 17O-labeled water in healthy subjects, the extent of CSF leakage captured by 17O-MRI may vary with age and disease and lead to an early imaging diagnosis of dementia. Intravenously administered 17O-labeled water is distributed in the brain parenchyma, and CBF measurements can be performed as previously mentioned.
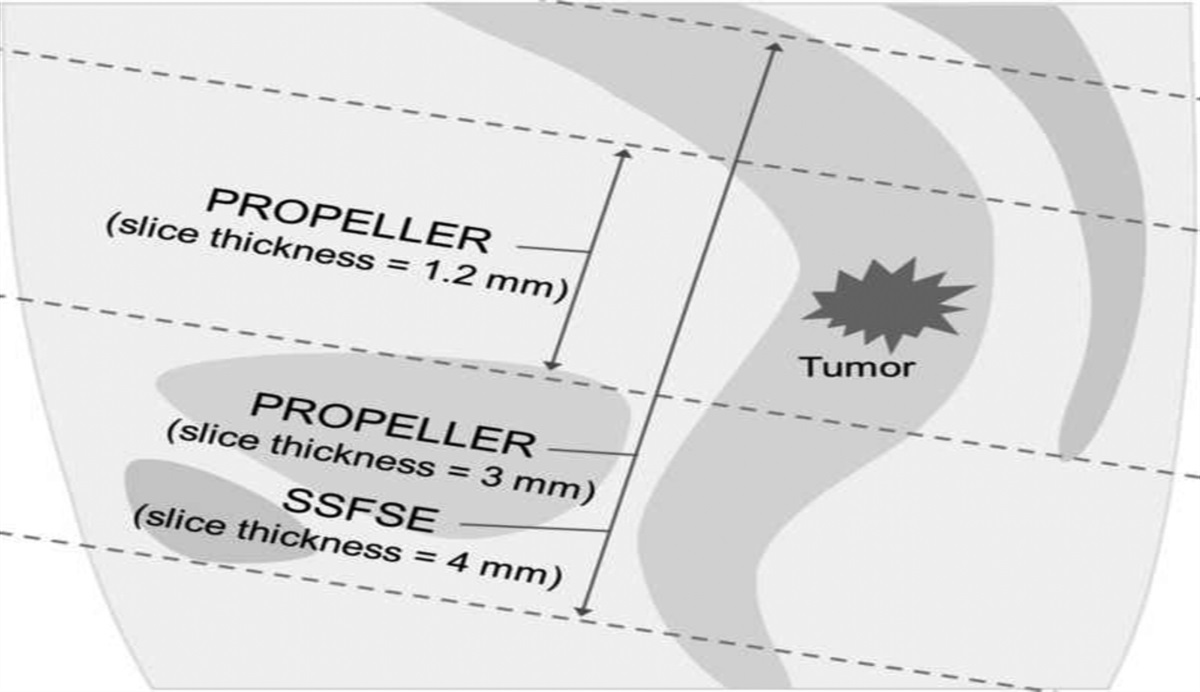
Classically, CSF is produced in the choroid plexus and absorbed by the arachnoid villi.119 However, recent studies using 17O-labeled water challenge this classical theory. Igarashi et al67 reported no significant differences between AQP-1 knockout and wild-type mice in signal changes in the CSF after intravenous administration of 17O-labeled water using the JJVCPE sequence, whereas AQP-4 knockout mice showed significantly reduced signal changes in the CSF. AQP-4 is the most abundant isoform, and its distribution is uniquely restricted to the subpial and perivascular endfeet of astrocytes, whereas AQP-1 is mainly expressed in the choroid plexus epithelium and AQP-4. Therefore, water influx into the CSF is regulated by AQP-4 and not by AQP-1 found in the choroid plexus, suggesting that water production in the CSF is not regulated by the choroid plexus. Another study showed earlier and larger signal changes in the subarachnoid space of the brain surface than in the ventricles after intravenous injection of 17O-labeled water using SSFP sequences, suggesting that more water in the CSF is produced in the subarachnoid space than in the choroid plexus of the ventricles (Fig. 2B).24 AQP-4 has also been shown to regulate water entry and exit at the blood-brain barrier using 17O-MRI.12017O-labeled water can elucidate CSF dynamics, particularly during production. In addition, it holds potential for molecular functional imaging of AQP-4.
Besides intravenous injections, intrathecal injections are another approach for measuring CSF dynamics. In animal studies, intrathecal administration of 17O-labeled water allowed the visualization of CSF dynamics (Fig. 6). Furthermore, this approach can be used to image the glymphatic system.121,12217O-labeled water can be injected into the CSF, and its movement through the glymphatic system can be imaged using MRI (Fig. 6A). Intrathecal injection of a Gd tracer into AQP-4 knockout (KO) rats alters the kinetics of Gd in the CSF compared with those in wild-type rats.123 According to a recent animal study, when 17O-labeled water (90% 17O enrichment) was injected into rat brain cisterns, the temporal migration of 17O from the CSF to the brain parenchyma was visualized using MRI and was more rapid and extensive than that of conventional Gd tracers; this distribution was inhibited by AQP-4 inhibitors.38 However, in this report, rodent studies must use highly concentrated 17O-labeled water (90% 17O enrichment) and higher SNR T2-weighted sequences to detect small signal changes in the brain parenchyma on proton MRI. This may be because of limitations on the rate and volume of tracers injected into rats to avoid increased intracranial pressure.
 FIGURE 6:
FIGURE 6: Dynamic 17O-MRI with intrathecal injection in preclinical studies. A, The 17O map derived from continuous T2WIs (TR/TE, 3000/100 milliseconds; echo train length, 16; thickness, 1.0 mm; in-plane resolution, 0.1 × 0.1 mm; time resolution, 30 seconds) with preclinical 7 T MRI, using intrathecal injection of 17O-labeled water (90 mol%, 10 μL, 0.5 μL/min) into the cisterna magna of the mouse. B, Evaluation of amyotrophic lateral sclerosis (ALS) model mice before and after onset of disease (11/16 weeks old) using 17O-MRI. Dynamic concentration changes of intrathecal H217O in the cerebellum (left and middle panel). Comparison of mean 17O concentrations from 900 to 1500 seconds after administration (right panel). WT, wild-type mice.
Gd contrast agents can visualize CSF dynamics; however, because of differences in molecular weight and chemical properties, their spatiotemporal scale is significantly different from that of 17O-labeled water. In addition, safety and efficacy studies on human intrathecal injection of Gd contrast agents are ongoing124,125; however, presently, intrathecal injection of Gd contrast agents is prohibited.
Diseases in which CSF dynamics, particularly the disruption of CSF turnover (production and absorption), are involved in the pathogenesis include AD and hydrocephalus. In amyotrophic lateral sclerosis (ALS), the blood–brain–spinal cord barrier is disrupted at an early stage, and communication between CSF and interstitial fluid through the perivascular space may be abnormal.126 After intrathecal injection of 17O-labeled water into ALS model mice, the amount of 17O-labeled water distributed in the cerebellum was significantly higher in the ALS group than in the control group (Fig. 6B). Moreover, a human study on dementia and idiopathic normal pressure hydrocephalus has been conducted.26 A preliminary study using a 3D-FSE sequence suggested that CSF clearance significantly differed between patients with dementia and those with hydrocephalus. In this study, patients with idiopathic normal pressure hydrocephalus showed delayed excretion of 17O-labeled water in the CSF compared with those with AD. However, T2WI was performed with a long TE targeting the CSF, which has a long T2 value, resulting in reduced SNR in regions with relatively short T2 values, such as the brain parenchyma, and thus, the distribution of 17O in the brain parenchyma was not properly detected. In a study using a shorter TE, 17O-labeled water dynamics administered through the lumbar route was visualized in the subarachnoid space, ventricle, and brain parenchyma (Fig. 7). A major advantage of 17O-MRI is the long-term follow-up of the distribution of water in the CSF to the brain parenchyma and other components of neurofluids. However, CSF dynamics can be influenced by various physiological factors such as respiration, heart rate,127–129 body position, sleep state (eg, sleep deprivation),130 and aging. These factors can lead to significant variations in CSF dynamics within individuals, emphasizing the need for a noninvasive and repeatable measurement method for evaluation. Thus, 17O-MRI, being a transient and invasive imaging method, has limitations, therefore combining this method with noninvasive CSF/neurofluids imaging techniques,90,131 such as diffusion-weighted imaging (diffusion tensor image analysis along the perivascular space),89,92,93,132 PC, and ASL,94 to understand the dynamics of neurofluids (Fig. 5).
 FIGURE 7:
FIGURE 7: CSF dynamics in humans after intrathecal injection of 17O-labeled saline. The distribution of 17O in the brain of a patient with suspected dementia after intrathecal administration of 17O-labeled saline (10 mol%, 10 mL). The 17O map was calculated by 3D fast spin echo T2WIs (before, 1 hour, 8 hours, and 24 hours after administration). In the CSF space, the concentration of 17O peaked 1 hour after administration. The distribution of 17O is particularly high in the bilateral Sylvian fissures. After that, the concentration tends to decrease.
Although some issues are still to be solved for human application, including the sensitivity and specificity of 17O detection, this imaging technique is considered new in terms of imaging diseases related to abnormal brain water dynamics, in addition to elucidating the mechanism of the glymphatic system. Many studies have been conducted on the mechanisms of the CNS fluid system surrounding the glymphatic system, which is becoming more complex and must be integrated in the future; 17O-MRI can help in this field.
Intraocular WaterThe anterior aqueous humor is a clear fluid that fills the anterior chamber of the eye, located between the cornea and lens. The aqueous humor provides nutrients to the cornea and lens and helps maintain intraocular pressure. The dynamics of the aqueous humor are important in diagnosing and treating various ocular diseases, such as glaucoma. In vivo animal and human MRI and MRS using 17O-labeled water or heavy water (D2O) have been used to examine aqueous humor dynamics. In a rabbit study, 17O-labeled water outflows were observed in the anterior chamber after the administration of 17O-labeled water eye drops by both indirect imaging using SE and direct imaging using MRS.56 Another in vivo human study showed an increase in 17O-labeled water concentration in the anterior chamber after the administration of 17O-labeled water eye drops, followed by a return to the concentration before the administration of the eye drops (Fig. 8).2817O-labeled water has also been intravenously administered to rabbits, and an increase in 17O-labeled water has been detected in the anterior chamber and lens.133 None of the aforementioned 17O-labeled water studies showed 17O-water–induced MR signal intensity changes in the vitreous body. However, a study reported the detection of heavy water in the vitreous body by direct deuterium imaging after the intravenous injection of heavy water in rabbits.134 The differences in these results might be because of the concentration of water, the difference in water properties caused by the bonding 2H or 17O, or the sensitivity of the imaging sequence. However, further studies are required to elucidate the difference in water dynamics between 17O-labeled water and heavy water, or between eye drops and intravenous solutions.
 FIGURE 8:
FIGURE 8: Intraocular water movement visualization with eye drops of 17O-labeled saline. Extreme left, the averaged T2WI obtained before H217O eye drop application (referred to as T2WI0, −0.75 to −0.25 minutes). Others, subtracted images. Each image was derived by subtracting the T2WI0 from the averaged T2WIx image obtained at x = 2.5–3.0, 8.5–9.0, or 40.5–41.0 minutes. The time point t = 0 is the end of the eye drop application. AC, anterior chamber; PC, posterior chamber; VB, vitreous body.
Articular FluidArticular fluid is a lubricating fluid that fills the synovial cavity of joints, provides nutrition to the articular cartilage, and reduces friction between bones. The dynamics of articular fluid are potentially important in diagnosing and treating of various joint diseases, such as osteoarthritis. Articular cartilage is another target of 17O-labeled water imaging because cartilage degeneration can be detected by the abnormal absorption of 17O-labeled water.
Hosokawa et al29 reported that early articular cartilage damage in rabbits after anterior cruciate ligament transection can be detected by the T2 FSE sequence after the administration of 17O-labeled water (20%) in the knee joint (Fig. 9). Signal changes in the articular cartilage were larger in the damaged area than in other parts of the cartilage, suggesting alterations in the hydrostatic pressure in the damaged cartilage. Therefore, this method can help in the early diagnosis of osteoarthritis. However, the diagnostic capabilities of this method have not yet been compared with those of existing MRI diagnostic techniques, such as T2 mapping, T2* mapping, T1rho mapping, and delayed Gd-enhanced MRI,135 which are commonly used for diagnosing osteoarthritis. Therefore, further validation is required to assess its diagnostic potential in the early detection and evaluation of osteoarthritis.
 FIGURE 9: Detection of early damage to the articular cartilage in rabbit knees by intraarticular administration of 17O-labeled water. A, Macrographs of rabbit knees after anterior cruciate ligament amputation, representing a model of knee osteoarthritis. Dashed yellow lines indicate the corresponding sections of tissue and MR image. B, Histological images with Safranin O Fast Green staining, where arrows indicate the articular cartilage lesions. C, 17O concentration maps of the articular cartilage region, calculated from signal values of T2 fast spin echo images acquired before and after intraarticular administration of 17O-labeled saline (10 mol%), fused with proton density-weighted images. This figure was previously presented by Hosokawa et al29 licensed under CC BY 4.0.Inner Ear
FIGURE 9: Detection of early damage to the articular cartilage in rabbit knees by intraarticular administration of 17O-labeled water. A, Macrographs of rabbit knees after anterior cruciate ligament amputation, representing a model of knee osteoarthritis. Dashed yellow lines indicate the corresponding sections of tissue and MR image. B, Histological images with Safranin O Fast Green staining, where arrows indicate the articular cartilage lesions. C, 17O concentration maps of the articular cartilage region, calculated from signal values of T2 fast spin echo images acquired before and after intraarticular administration of 17O-labeled saline (10 mol%), fused with proton density-weighted images. This figure was previously presented by Hosokawa et al29 licensed under CC BY 4.0.Inner Ear
Endolymph is a fluid found in the inner ear and plays a crucial role in maintaining balance and hearing. Investigating the endolymph by imaging is important because its abnormalities can lead to various hearing and balance disorders, such as Meniere disease, characterized by endolymphatic hydrops.
Recently, Yoshida et al30 first reported the intratympanic administration of 17O-labeled water in 5 healthy subjects and 1 patient with endolymphatic hydrops. They used the indirect method (heavily T2 MR hydrography) with proton MRI and demonstrated that 17O-labeled water permeated the cochlear basal turn and vestibule at 30 minutes and disappeared gradually within 2–4 hours. However, all participants experienced positional vertigo lasting from a few hours to a few days, which might be a potential drawback of this local injection method.
Other OrgansMyocardial blood flow assessment is an equally important research topic as CBF assessment, and 17O-labeled water holds potential for such evaluation. Borowiak et al42 reported the ability to visualize naturally occurring 17O in human myocardial tissue with a temporal resolution of 200 milliseconds using a direct method using electrocardiogram-gated 3D-UTE radial pulse sequences in clinical 3 T MRI. Furthermore, other groups demonstrated the evaluation of myocardial oxygen consumption by detecting 17O-labeled water, produced because of metabolism in myocardial mitochondria, through direct methods in ex vivo rat hearts (using direct 17O-MRI)136 and in vivo dogs (using the indirect method involving T1ρ imaging).137 To date, no studies have evaluated myocardial blood flow using in vivo administration of 17O-labeled water, likely because of cost considerations. The myocardial region poses challenges because of acquisition time limitations associated with the cardiac cycle, and currently, techniques directly applicable in clinical practice are limited. However, as the clinical applications of 17O-MRI in the neuroimaging field advance, an increase in future studies addressing this aspect is anticipated.
The kidney is as a vital organ in diagnosing numerous diseases and conditions, due to its unique evaluation parameters such as renal blood flow and glomerular filtration rate. Despite its significance, the application of 17O-labeled water and MRI in vivo for kidney assessment remains unexplored in current literature. Addressing this research gap, Campos Pamplona et al138 conducted a study using a clinical 3 T MRI system and a 17O 3D-UTE sequence, providing valuable insights into the dynamic evaluation of 17O-labeled metabolic water as a potential tool for assessing the quality of transplanted kidneys. Their findings hold promise for future advancements in the field of kidney evaluation and warrant further investigation in clinical settings.
FUTURE CHALLENGES AND PERSPECTIVESWater imaging techniques using 17O-labeled water and MRI have been attempted to visualize the water dynamics of various organs, such as brain blood flow, CSF dynamics, eyeball, inner lymphatics, articular cartilage, and myocardial blood flow, resulting in the generation of MR images with a new clinical value. However, several challenges remain.
Regarding the clinical use of 17O-labeled water, a significant issue with cost arises, depending on the administration route. Furthermore, a sensitivity issue should be mentioned, and increasing the concentration and dose of 17O-labeled water is highly anticipated in 17O-MRI.
In MRI, as mentioned earlier, recent advancements have been made in the biological applications of 17O-labeled water detection using indirect methods, including proton MRI that involving human subjects. Compared with direct methods, which have lower sensitivity because of the use of less sensitive 17O, indirect methods enable high sensitivity 17O-labeled water imaging and are widely applicable on commonly available clinical MRI devices, thus offering widespread applicability. However, in a low concentration range, the noise is higher, decreasing accuracy. In addition, indirect methods are affected by various external factors, such as fluctuations in B0 or B1 and various artifacts, and internal factors, such as motion and changes in the vascular bed and oxygen concentration, resulting in low 17O specificity. In contrast, the clinical application of direct methods has mainly relied on the use of oxygen gas in the past, and the application of 17O-labeled water has lagged. Although direct methods have sensitivity issues, recent studies have demonstrated the detection of naturally occurring 17O in the human brain and heart on clinical 3 T MRI.42 highlighting the need to further investigate the effectiveness of 17O-labeled water even with direct methods.
In the future, it is anticipated that, while verifying the feasibility and validity of direct methods for the effectiveness of 17O-labeled water imaging demonstrated by indirect methods, water dynamics evaluation of other organs (eg, breast, liver, gallbladder, pancreas, gastrointestinal tract, and prostate) and tumor water dynamics evaluation, as well as molecular functional imaging of AQP-4 and others, will be developed. Furthermore, although it is not the focus of this review, technological innovations regarding 17O enrichment and large-scale production are also expected in this field.
In conclusion, 17O-MRI is used to visualize blood flow and water dynamics in various organs, such as the CSF, cerebral interstitial fluid flow (neurofluids), eye, articular cartilage, and endolymph. This method is expected to be used to establish new diagnostic imaging methods for CNS diseases and other disorders in the future.
REFERENCES 1. Rasmussen MK, Mestre H, Nedergaard M. Fluid transport in the brain. Physiol Rev. 2022;102:1025–1151. 2. Weiskopf N, Edwards LJ, Helms G, et al. Quantitative magnetic resonance imaging of brain anatomy and in vivo histology. Nature Reviews Physics. 2021;3:570–588. 3. Williamson NH, Komlosh ME, Benjamini D
Comments (0)