Study Design
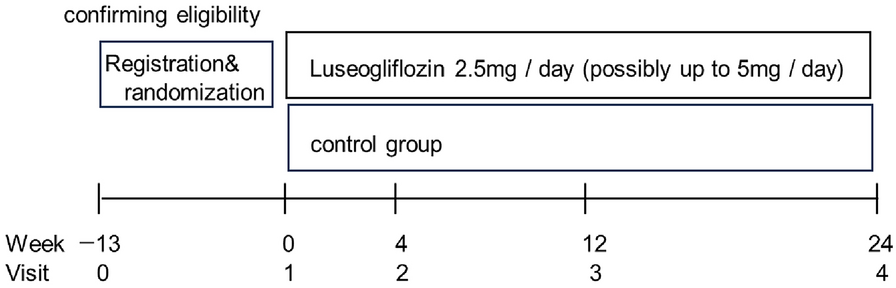
To compare treatment effectiveness and durability of semaglutide and DPP–4i in persistent users, this observational cohort study used deidentified data collected from the Optum® Clinformatics® Data Mart (CDM) between January 1, 2017 and September 30, 2022 (end of study; Supplementary Fig. 1). The index date (day 0) was defined as the new initiation date of the index drug (semaglutide or a DPP–4i). The selection window for initiation of the index drug was from January 1, 2018 to 720 days before the end of the study. The baseline period was defined as 1 year before the index date [days − 360, − 1]. Outcomes were assessed in the 2-year follow-up period from the index date to 719 days after the index date [days 0, 719].
Data Source
The Optum® CDM is a database containing administrative claims data for a large managed care population, including commercial and Medicare Advantage health plan members from geographically diverse regions of the USA. Longitudinal medical and pharmacy claims data in the Optum® CDM are verified, adjudicated, adjusted, and deidentified and include information on patient demographics, inpatient and outpatient medical care, pharmacy dispensing, and outpatient laboratory test results from national laboratory vendors.
Study Population
Individuals aged ≥ 18 years were eligible on the basis of their having a pharmacy claim for an index drug (semaglutide or DPP–4i) during the index date selection window (January 1, 2018 to October 10, 2020) and their having a confirmed T2D diagnosis, defined as ≥ 2 claims for International Classification of Diseases, Tenth Revision, Clinical Modification (ICD-10-CM) code on distinct days between January 1, 2017 and September 30, 2022, with ≥ 1 record during the baseline period. DPP–4is included in this analysis were sitagliptin, saxagliptin, linagliptin, and alogliptin. Individuals were required to have continuous enrollment for 360 days before index date and 719 days after index date as well as persistent use of index drug for ≥ 720 days, defined as ≤ 90-day gap from the date of first pharmacy claim to exhaustion of days’ supply of the last pharmacy claim. For individuals in the DPP–4i cohort, switching in the same drug class during the follow-up was allowed. Exclusion criteria included diagnosis of type 1 diabetes, pregnancy, use of any GLP-1 RA or DPP–4i during the baseline period, use of ≥ 2 types of products in the index drug class on the index date, initiation of another new glucose-lowering drug class on the index date, bariatric surgery, or use of antiobesity medications during the study period.
As a result of data availability and limited sample size, two cohorts were analyzed in this study: the HbA1c cohort and the BMI cohort. The HbA1c cohort was composed of individuals with HbA1c values available in the dataset at baseline (between 120 and 1 days before the index date) and follow-up (between 540 and 719 days after the index date). The BMI cohort was composed of individuals with BMI values available at baseline (between 180 and 1 days before the index date) and follow-up (between 540 and 719 days after the index date).
Outcome and Covariates Measures
Primary HbA1c outcomes were measured for the HbA1c cohort and included HbA1c level at 2-year follow-up, change in HbA1c level from baseline to follow-up, and proportion of individuals achieving HbA1c levels < 7% and < 8% in the follow-up period. Exploratory treatment augmentation outcomes were also measured for the HbA1c cohort. Time to treatment augmentation was measured as the duration from day 60 to the date of adding a new glucose-lowering drug class that was neither the index drug class nor the treatment used at baseline; ≥ 2 prescription claims for the new glucose-lowering drug starting at least 60 days before the last date of the index drug or the end of study, whichever came first, were required. In the subset of individuals who did not use insulin before day 60, the time to insulin initiation was also explored; ≥ 2 prescription claims for insulin initiated at least 60 days before the last date of the index drug or the end of study, whichever came first, were required.
For the BMI cohort, exploratory BMI outcomes were measured using ICD-10-CM codes and included change in BMI from baseline to follow-up and proportion of individuals with decreasing BMI category from baseline to follow-up. In this study, BMI values were defined as the midpoint of the ICD-10-CM code (e.g., ICD-10-CM code Z68.25 [adult BMI 25.0–25.9 kg/m2] was defined as BMI 25.45 kg/m2 in this study). BMI categories were defined as < 25, 25 to < 30, 30 to < 35, 35 to < 40, and ≥ 40.
Covariates included age, sex, race and ethnicity, geographic region, index year, payer type, insurance plan type, prescriber specialty, Charlson Comorbidity Index (CCI; CDMF version) [17, 18], Diabetes Complication Severity Index (DCSI) [19, 20], common comorbidities (yes/no), common concomitant drug classes (yes/no), diseases/conditions related to weight changes, medications associated with weight gain (yes/no), number of glucose-lowering medications, glucose-lowering drug class at baseline, common procedures (yes/no), number of all-cause hospitalizations (60 days before index date), number of all-cause emergency department visits (60 days before index date), baseline out-of-pocket costs for all prescription drugs, and number of follow-up days amid the COVID-19 pandemic (i.e., follow-up days after March 1, 2020).
Statistical Analyses
Descriptive analyses were conducted in both semaglutide and DPP–4i groups. Counts and frequencies were used for categorical variables; means and SDs, for continuous variables.
To reduce the selection bias and observed confounding between the two groups, inverse probability of treatment weighting (IPTW) [21] was derived by conducting a regularized logistic regression with elastic net penalty on the semaglutide group vs DPP–4i group with the following variables: age, race and ethnicity, index year, payer type, CCI, DCSI, glucose-lowering medications, baseline HbA1c level, baseline BMI and obesity diagnosis, health care utilization at baseline, comorbidities, and other medications at baseline. The targeted average treatment effect estimate was unable to be sufficiently balanced; therefore, the average treatment effect of the treated (ATT) was estimated. For all covariates, descriptive statistics were reported with and without IPTWs. Standardized mean differences (SMDs) were presented, and SMD ≥ 0.1 was considered a meaningful difference. Weighted descriptive statistics, bivariate analyses, and multivariate analyses were conducted. Both bivariate analyses and multivariate analyses used linear and logistic regression models with robust SEs. Bivariate analyses were conducted without adjusting for covariates (reported as unadjusted), while multivariate analyses also controlled covariates that were not balanced between groups (reported as adjusted). For time-to-event outcomes, weighted Kaplan–Meier cumulative incidence function and log-rank test statistic, as well as Cox proportional hazards (PH) regression with robust SEs, were used.
Two subgroup analyses were also explored: those with baseline HbA1c ≥ 7.0% and those whose treatment escalated to 1 mg semaglutide in their last dose before the follow-up HbA1c or BMI measures. Subgroup analyses were not reweighted between the subgroup of semaglutide and DPP–4i users, and only bivariate analyses were conducted in subgroup analyses. A sensitivity analysis of main outcomes using 1:1 ratio propensity score matching (PSM) was also conducted. All analyses were performed using R 4.0.4.
Compliance with Ethics Guidelines
The claims data assessed were in accordance with Health Insurance Portability and Accountability Act. This study was exempt from institutional review board review because this study was not classified as research involving human subjects. Database access and use of the data analyzed in this study were permitted by Optum® Clinformatics®. This study was performed in accordance with the Helsinki Declaration of 1964 and its later amendments. All authors meet the International Committee of Medical Journal Editors criteria for authorship for this article, take responsibility for the integrity of the work as a whole, and have given their approval for the version to be published.



留言 (0)