
記住我
Inappropriately managed postoperative pain is associated with a broad range of negative consequences, including increased morbidity, reduced quality of life, prolonged hospital length of stay, and increased risk of chronic postoperative pain.1 Epidural analgesia is a well established practice in thoracic surgery for optimal pain relief2 and improved quality of life.3 It provides better pain relief and preserves postoperative pulmonary function compared with systemic opioids during conventional thoracotomy.4
Acute pain after video-assisted thoracic surgery (VATS) is often perceived as less severe than that after open thoracotomy,5,6 but there is no consensus on the best perioperative pain management after VATS.7 Most recommendations primarily discuss using different loco-regional techniques as part of a multimodal approach to postoperative pain management.8,9 The possibility of omitting regional analgesia altogether, thus eliminating any risk of procedural complications, is seldom discussed, apart from the desire to avoid opioids due to possible adverse effects.8,9
The evidence supporting epidural analgesia over systemic opioids for pain management after VATS is inconclusive. The current literature includes three observational studies10–12 and three RCTs,13–15 all small and non-blinded. The results are conflicting, as some studies demonstrated a superior effect of epidural analgesia,14,15 whereas others did not show any additional effect compared with oral morphine.10–13 Consequently, current reviews emphasise the need for further studies in this area of research.16–18 The standard practice for postoperative pain management after VATS in our department is a multimodal approach with non-opioid baseline analgesia supplemented with perioperative intercostal blocks and an epidural catheter is used while the chest drain remains in place.
We hypothesised that it may be possible to reduce postoperative pain by switching from epidural analgesia to oral opioids. Using a double-blind approach, our aim was to compare postoperative pain after VATS using either epidural analgesia or oral morphine as part of a multimodal approach to postoperative pain management.
Methods Study design and participantsWe performed a patient- and observer-blind, parallel-arm, randomised controlled trial at a public university-based cardiothoracic anaesthesia and surgery department at Odense University Hospital, Odense, Denmark. The study was conducted in accordance with the Helsinki Declaration, was approved by The Regional Scientific Ethical Committees for Southern Denmark (project ID: S-20140035, 01/29/2018, chairperson JM Hertz), registered with ClinicalTrials.gov (NCT02359175) and monitored for data quality by The Good Clinical Practice Unit of Southern Denmark. The trial protocol is available upon request. We included patients over 18 years of age scheduled for elective VATS lobectomy, wedge, or segmental parenchymal resection due to known or suspected lung cancer who were willing to participate and accept epidural analgesia. Written consent was obtained if inclusion in the study was possible. The exclusion criteria were contraindications to using any trial medication or placement of an epidural catheter, chronic pain, or pregnancy.
Randomisation and maskingThe hospital pharmacy created a computer-generated randomisation list from a validated source (www.randomization.com) and provided consecutively numbered prepacked boxes with blinded study medication using block randomisation with blocks of four and treatment to placebo allocation 1 : 1. Packaging and all study medications (epidural infusions and tablets) were similar in appearance.
ProceduresOn the day of surgery, as per the standard procedure at our department, we placed a mid-thoracic epidural catheter at level T5–T6 using either the loss of resistance or the hanging drop technique at the physician's discretion. After placement and negative aspiration of blood or cerebrospinal fluid, we injected a test dose of 2–3 ml lidocaine (20 mg ml−1) with adrenalin (5 mcg ml−1) to verify the clinical effect before general anaesthesia. After inserting the epidural catheter, the anaesthetist allocated the patients to the next sequential randomisation number and administered oral premedication: paracetamol (1 g), ibuprofen (400 mg) along with the blinded study medication (placebo or oral morphine 10 mg). General anaesthesia was induced and maintained with propofol and remifentanil in conjunction with an epidural infusion of bupivacaine (2.5 mg ml−1) containing sufentanil (1.0 mcg ml−1). Supplementary intravenous fentanyl was used during surgery at the anaesthetist's discretion. All patients received a double-lumen endotracheal tube for one-lung ventilation, and VATS was performed as a nonrib-spreading procedure using the lateral decubitus position. At the end of the surgery, all patients received intercostal blockades (bupivacaine 2.5 mg ml−1, 20 ml), subcutaneous infiltration of the surgical wounds (bupivacaine 2.5 mg ml−1, 10 ml), and had a 24F chest drain inserted. Postoperatively, the patients went to the post-anaesthesia care unit (PACU), where a nurse set up the patient controlled epidural analgesia (PCEA) pump, replacing the intra-operative epidural medication with the blinded study infusion – either 0.9% normal saline or bupivacaine 1.0 mg ml−1 with fentanyl 2.0 mcg ml−1. Baseline analgesics, consisting of paracetamol (1 g × 4), ibuprofen (400 mg × 3) and the blinded study medication (placebo or oral morphine 10 mg) supplemented with the blinded solution for epidural infusion, continued throughout the study. On-demand intravenous rescue morphine was available to all patients during the study period. We set the initial epidural infusion rate after surgery according to the patient's height (<165 cm: 5 ml h−1 with a patient administered bolus dose of 3 ml, otherwise 7 ml h−1and a bolus of 4 ml, and a lockout time of 20 min), with the option of subsequent changes to the background infusion by the ward nurse if necessary. We recorded the use of all trial medications. If a test of correct epidural catheter placement was needed, a predefined bolus of lidocaine according to the patient's height was used, and efficacy was tested using cold sensations in the relevant dermatomes. Throughout the study, we evaluated pain using the 11-point Numeric Rating Scale (NRS), where a score of 0 represented “no pain” and a score of 10 described “worst pain imaginable.” NRS (rest) was defined as the pain experienced by the patient at rest at the time of the assessment, and NRS (activity) was defined as the pain experienced upon mobilisation or coughing. For clinical relevance, we categorised NRS scores as “acceptable pain” and “unacceptable pain,” defining “unacceptable” pain that would require supplementary analgesic as NRS (rest) ≥3 and NRS (activity) ≥5.
In the PACU, the pain was evaluated at rest on admission and discharge using the four-point categorised pain scores recommended by the Danish Society of Anaesthesiology and Intensive Care Medicine.19 In the surgical ward, we recorded postoperative pain for the first four days after surgery using NRS scores five times daily (6 a.m., 10 a.m., 2 p.m., 6 p.m., and 10 p.m.) at rest and during activity. The patients did all pain assessments assisted by a ward nurse. The study was terminated upon the concurrent removal of the chest drain and epidural catheter as per the standard of care in our department, or on the fifth postoperative day at the latest.
OutcomesThe primary outcome measures were postoperative pain assessed as the proportion of patients experiencing “unacceptable pain” at least once during the study period, and the total consumption of intravenous “rescue” morphine in the surgical ward. The secondary outcome measures relevant to this study were the length of hospital stay and the possible side effects of epidural analgesia and systemic opioids. The recorded side effects were pruritus, dizziness, nausea, or vomiting. Episodes of hypotension (systolic blood pressure < 100 mmHg) and desaturation (oxygen saturation < 92% without supplemental oxygen) were recorded. The first postoperative voiding of urine or a bowel movement was recorded from the patient's chart.
Statistical analysisWe aimed to detect a 20% difference in the proportion of patients experiencing “unacceptable pain” at least once during the study period, assuming a 10% technical failure rate in the control group.20 Using an alpha value of 5% and power of 80%, a sample size of 124 patients was required. Initially, we experienced a high dropout rate due to higher than expected conversion to open thoracotomy, and randomisation was extended to include 161 patients. An external statistician performed an interim analysis of the primary outcome of pain after including the first 57 patients in the trial, upholding the blinded design by designating the treatment groups simply as Group 1 and Group 2. The analysis showed no significant between-group difference in pain giving no reason for premature termination of patient inclusion.
The primary and secondary endpoints were analysed using a modified intention-to-treat approach, excluding patients whose surgery was converted from the planned VATS to open thoracotomy. The primary outcome of pain was analysed using the chi-square test of homogeneity to examine the difference in the proportion of patients experiencing “unacceptable pain” at least once during the study period. We compared total morphine consumption between the two treatment groups during the study period using a two-sample Wilcoxon rank-sum test. For the secondary outcome measure, we used a Kaplan–Meier plot to illustrate the probability of still being in hospital and a Cox proportional hazards regression to obtain an estimate of the hazard ratio (HR). Fisher's exact test examined between-group differences in the recorded side effects. Summary statistics are presented as number (%) or as mean ± standard deviation. We undertook post hoc regression analyses using linear mixed models, including relevant covariates and accounting for nesting due to repeated measures. Model fit was examined visually using qq-plots of the residuals to check for normality. The post hoc analysis of hospital length of stay included added covariates to the Cox regression. We used the covariates age and sex in all posthoc regression models. In contrast, “time since surgery”, “time of day”, “pain at discharge from the PACU”, “morphine use in the PACU” and patient height were used only in the models to which they were perceived to have any clinical relevance. Regression effect estimates are given as means [95% confidence interval (CI), and P-values]. All analyses were performed with “R”21 and Stata/BE (StataCorp LLC, TX, USA) software, without imputation or stratification using two-sided P-values
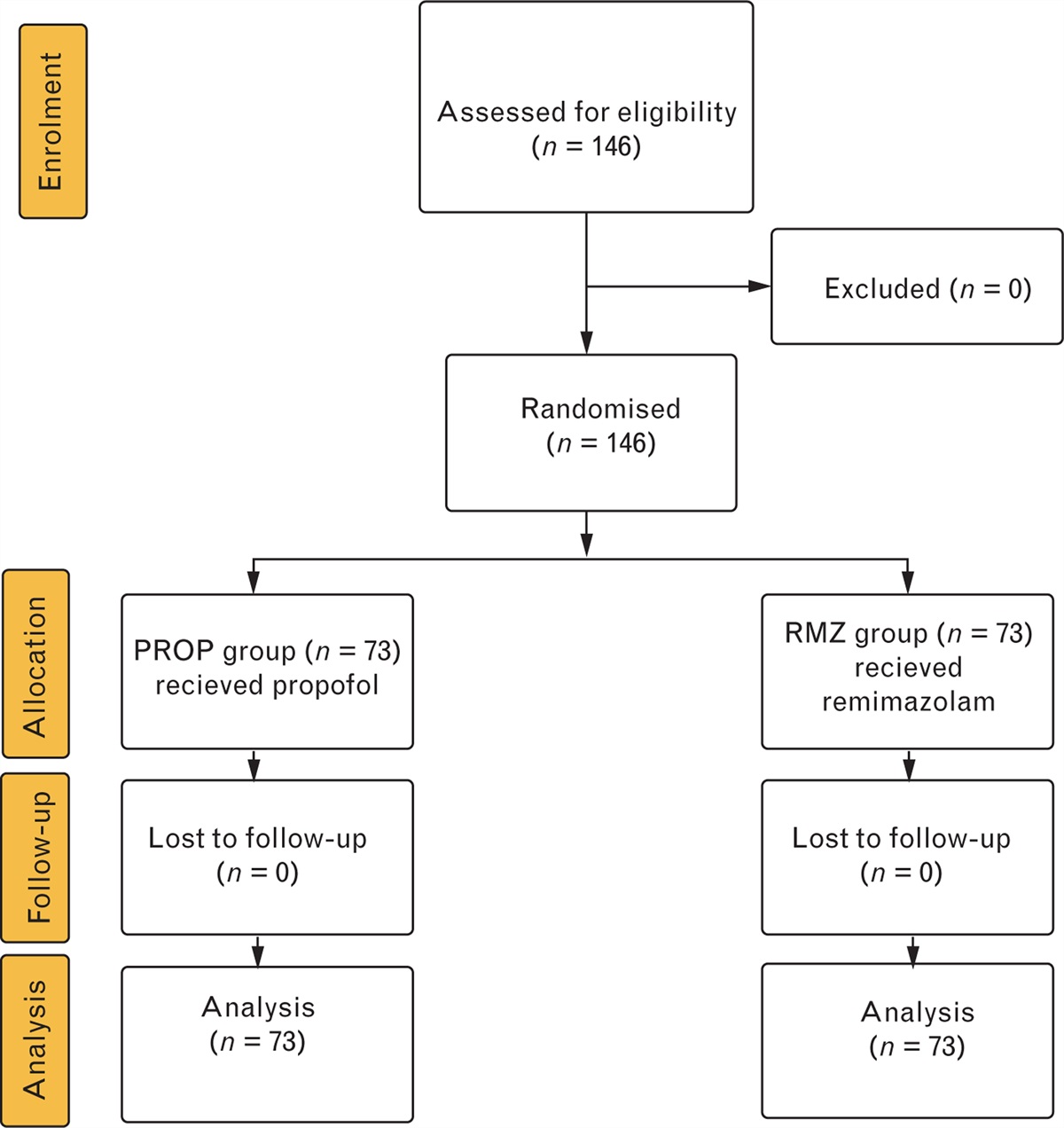
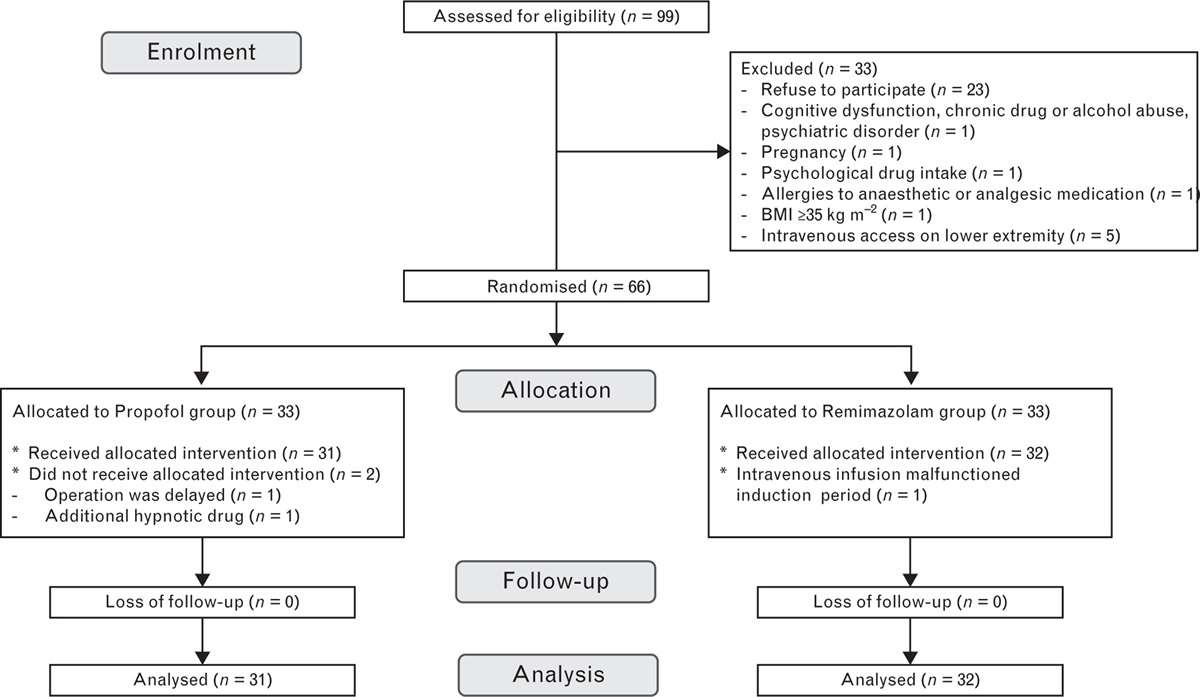
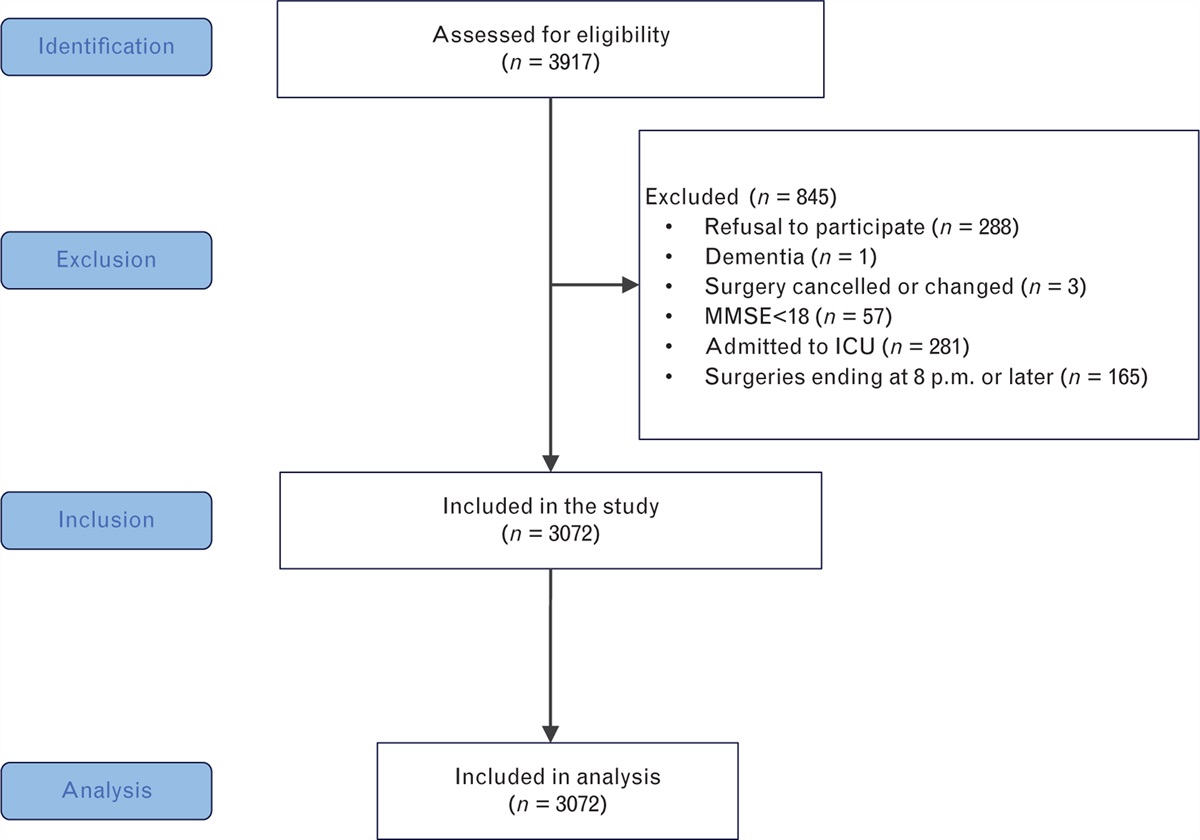
ResultsWe screened 810 patients with known or suspected pulmonary neoplasms scheduled for possible elective VATS lobectomy, wedge- or segmental resection from 30 April 2015 to 14 December 017. As shown in Fig. 1, we excluded 649 patients following the predefined inclusion and exclusion criteria, leaving 161 patients for randomisation. Of these, 15 did not receive the intended intervention because the surgical approach was changed to thoracotomy after allocation. Twenty-two patients discontinued the allocated intervention during the study. Three patients accidentally removed their epidural catheters, and the surgeon inadvertently removed one. One catheter was removed due to peri-catheter leakage, and three were discontinued at the patient's request. Four patients were excluded due to elevated creatinine levels, two because of gastrointestinal symptoms, six because of administrative faults, and two requested to be excluded because of nausea, leaving 124 patients who completed the entire trial period. Due to the chosen modified intention-to-treat approach, all patients receiving the allocated treatment (n = 146) were included in the analyses in the originally assigned group. Patient characteristics and anaesthetic and surgical data are shown in Table 1.
 Fig. 1:
Fig. 1: Participant flow.
Table 1 - Baseline demographics, anaesthetic and surgical data TE Group (n = 72) OM Group (n = 74) Patient demographics Age, years 68.5 ± 7.8 68.8 ± 7.5 Sex Male 36 (50) 38 (51) Female 36 (50) 36 (49) Height, cm 171 ± 10 170 ± 8 Bodyweight, kg 76 ± 12 77 ± 16 BMI, kg/m2 26 ± 4 27 ± 5 Ethnicity (Danish) 72 (100) 74 (100) ASA Classification ASA I 0 2 (3) ASA II 37 (51) 46 (62) ASA III 35 (49) 26 (35) ASA IV 0 0 ASA V 0 0 Peroperative anaesthetic data Propofol infusion (mg) 1078 ± 706 1048 ± 835 Remifentanil infusion (mcg) 1906 ± 916 2068 ± 1048 Bolus fentanyl (mcg) 39 ± 58 51 ± 77 Epidural infusion (ml) 14 ± 7 14 ± 5 Surgical data Type of surgery Lobectomy 54 (75) 57 (77) Wedge resection 15 (21) 15 (20) Segmental resection 3 (4) 2 (3) Duration of surgery (min) Lobectomy 102 ± 26 103 ± 26 Wedge resection 50 ± 28 42 ± 20 Segmental resection 85 ± 10 105 ± 9 Surgical ports One 7 (10) 9 (12) Two 20 (28) 17 (23) Three 45 (63) 47 (64) Four 0 1 (1) Post-anaesthesia care unit Admittance pain score 0 39 (54) 46 (62) 1 9 (13) 10 (14) 2 16 (22) 9 (12) 3 16 (10) 9 (12) Missing 1 (1) 0 Discharge pain score 0 35 (49) 43 (58) 1 35 (49) 30 (41) 2 1 (1) 1 (1) 3 0 0 Missing 1 (1) 0Baseline characteristics and perioperative summary statistics for the trial patients by randomisation group in the intention-to-treat population (n = 146). Data are n (%) and mean ± SD.ASA, American Society of Anesthesiologists; TE Group, thoracic epidural group; OM Group, oral morphine group.
The proportions of “unacceptable” pain during the trial period in the two treatment groups are depicted in Fig. 2. At rest, 23 of the 68 patients (34%) in the TE Group and 44 of the 69 patients (64%) in the OM Group experienced unacceptable pain, with a significant between-group difference of 30%, χ2 (1, n = 137) = 12.3, P < 0.0005. During activity, these values were 22 of 68 (32%) in the TE Group and 41 of 69 (59%) in the OM group, a significant difference of 27%, χ2 (1, n = 137) = 10.1, P = 0.001. The pain scores across all time points for both treatment groups are shown in Fig. 3.
 Fig. 2:
Fig. 2: Frequency of unacceptable pain.
 Fig. 3:
Fig. 3: Summary statistics of pain scores.
The median dose of intravenous rescue morphine during the study period was 4.5 [interquartile range (IQR) 0–10.0] mg in the TE Group and 7.5 [0 to 19.0) mg in the OM Group (z = 4.294, P < 0.001).
We found no difference in the length of hospital stay between the study groups: hazard ratio (HR), 0.97 (95% CI, 0.70–1.34), P = 0.8).
We did not see any differences in the recorded side effects between the two groups (P > 0.054). A full description of the side effects possibly related to the use of an epidural catheter or opioids (pruritus, hypotension, desaturation, dizziness, nausea, vomiting, urinary retention or ileus) is available in the supplementary material, https://links.lww.com/EJA/A885.
The post hoc regression analyses of the primary and secondary outcomes are shown in Table 2. Pain scores across all time points during the trial showed significantly higher scores with oral morphine compared with epidural analgesia. These differences were present both at rest and during activity. Compared to the TE Group, the mean NRS score in the OM Group was 1.0 point higher at rest (95% CI 0.6–1.4, P < 0.001) and 1.3 points higher during activity (95% CI 0.8–1.9, P < 0.001). Time since surgery, time of day, and the pain level at discharge from the PACU were significant covariates, except for the pain score at rest on POD1 and for patients with a discharge pain score of two. Age and sex were not significant covariates in the model, neither at rest nor during activity. A figure of pain score across all time points as estimated by regression is depicted in Fig. 4. Regarding the use of “rescue” morphine, the regression analysis showed a significant difference between groups with patients in the OM Group using 1.7 mg per day more morphine than those in the TE Group (95% CI 0.9–2.4, P < 0.001). Age (P = 0.012) and “time since surgery” were significant covariates for the amount of “rescue” morphine used during the postoperative period: sex and morphine consumption in the PACU were not significant covariates. For the hospital length-of-stay, adding the chosen covariates to the Cox proportional hazards model did not change the result (adjusted HR: 1.02, 95% CI 0.73–1.41, P = 0.9).
Table 2 - Regression analyses for the primary and secondary outcome measures Regression coefficient P value Pain scores (NRS), at rest Intercept 2.2 (0.2 to 4.1) 0.029 OM Group 1.0 (0.6 to 1.4) < 0.001 Age −0.0 (−0.0 to 0.0) 0.495 Sex (male) −0.2 (−0.6 to 0.2) 0.406 Time since surgery POD 0 (base) 0 POD 1 −0.3 (−0.6 to 0.0) 0.050 POD 2 −0.7 (−1.0 to −0.3) < 0.001 POD 3 −0.6 (−1.0 to −0.2) 0.002 POD 4 −0.8 (−1.5 to −0.0) 0.036 Time of day 6 am (base) 0 10 am −0.7 (−0.9 to −0.4) < 0.001 2 pm −0.7 (−1.0 to −0.4) < 0.001 6 pm −0.8 (−1.1 to −0.5) < 0.001 10 pm −0.8 (−1.2 to −0.5) < 0.001 Pain score, PACU Pain score 0 (base) 0 Pain score 1 0.7 (0.3 to 1.1) 0.001 Pain score 2 1.8 (−0.0 to 3.6) 0.051 Pain score 3 n/a n/a Pain scores (NRS), during activity Intercept 4.5 (1.8 to 7.1) 0.001 OM Group 1.3 (0.8 to 1.9) < 0.001 Age −0.0 (−0.1 to 0.0) 0.301 Sex (male) −0.4 (−0.9 to 0.2) 0.210 Time since surgery POD 0 (base) 0 POD 1 −0.7 (−1.0 to −0.4) < 0.001 POD 2 −1.1 (−1.5 to −0.7) < 0.001 POD 3 −1.3 (−1.8 to −0.8) < 0.001 POD 4 −2.1 (−2.9 to −1.2) < 0.001 Time of day 6 am (base) 0 10 am −1.0 (−1.3 to −0.6) < 0.001 2 pm −1.3 (−1.6 to −0.9) < 0.001 6 pm −1.5 (−1.9 to −1.2) < 0.001 10 pm −1.6 (−2.0 to −1.3) < 0.001 Pain score, PACU Pain score 0 0 Pain score 1 1.0 (0.5 to 1.6) < 0.001 Pain score 2 2.6 (0.0 to 5.1) 0.048 Pain score 3 n/a n/a Use of “rescue” morphine (mg) Intercept 4.0 (0.4 to 7.5) 0.028 OM Group 1.7 (0.9 to 2.4) < 0.001 Age −0.1 (−0.1 to −0.0) 0.012 Sex (male) 0.4 (−0.3 to 1.2) 0.265 Time since surgery POD 0 (base) 0 POD 1 1.5 (0.7 to 2.3) < 0.001 POD 2 0.6 (−0.5 to 1.6) 0.305 POD 3 1.0 (−0.3 to 2.4) 0.122 POD 4 −0.6 (−2.2 to 1.0) 0.493 Morphine use in the PACU 0.0 (−0.0 to 0.0) 0.558Results from multivariate mixed model regression analyses for the primary and secondary outcome measures. Data are regression coefficients (95% CI). Statistically significant P values are highlighted in bold. “Pain score, PACU” is the pain score recorded at discharge from the PACU. No patients were discharged with a pain score of three.POD, post-operative day; PACU, post-anaesthesia care unit. OM Group, oral morphine group.
 Fig. 4:
Fig. 4: Regression analysis.
The trial was concluded without any patients experiencing serious adverse events or reactions.
DiscussionIn our study, patients using oral morphine for postoperative pain management after VATS experienced significantly more pain than those using epidural analgesia. Additionally, the consumption of intravenous rescue morphine was significantly higher in the group that received oral opioids. With numbers-needed-to-treat (NNT) defined as 1/attributable risk reduction, the corresponding NNTs were 3.3 at rest (95% CI 2.2–7.2) and 3.7 during activity (2.3–9.1), indicating one additional patient experiencing “unacceptable” pain for every four patients treated with oral morphine for postoperative pain management after VATS compared with epidural analgesia. These results were consistent both when analysing results as crude between-group differences using condensed data and when using advanced regression analyses including random-effects and adjusting for repeated measures. When analysed across all time points during the five-day study period, we saw significantly more pain in the OM Group than the TE Group, with differences in mean NRS scores of 1.0 at rest and 1.3 during activity. This is in line with what is known for conventional thoracotomy, where epidural blockade provides better pain relief than systemic opioids,2,3 and aligns with the results from earlier studies indicating this might also be true for VATS.12,14,15 The present study adds significantly to this debate with a significant sample size, a blinded design, and a more comprehensive measurement of pain than previous studies.13–15 A reduction in pain intensity of 1.3 on the NRS scale22–24 or 1.0 on the Visual Analogue Scale25 is said to be clinically significant. By this definition, in addition to being statistically significant, the additional postoperative pain seen in our study when using oral morphine constitutes a clinically relevant increase.
We used the covariates of age, sex, and time since surgery in all models as they have been shown to influence pain perception.26–28 Time of day, pain at discharge from the PACU, and morphine use in the PACU were used only in the models to which they were perceived to have any clinical relevance.27 In our study, regression analysis showed the use of rescue opioids to be significantly higher among patients who received oral morphine compared with managing pain using epidural analgesia. The observed difference of an additional 1.7 mg per day of rescue morphine in the OM group, although statistically significant, is unlikely to constitute a clinically relevant difference. Our study found no differences in the hospital length-of-stay between the two groups, which aligns with previous comparable studies.10,15 With a significant sample size, a blinded design, and a more comprehensive pain measurement than previous studies, this trial supports the superior effect of epidural analgesia over systemic opioids for postoperative pain management after VATS.
Our study has some limitations that warrant consideration. First, we used a modified ITT approach for data analysis, deviating from a strict ITT approach by the post-randomisation exclusion of 15 patients after conversion to thoracotomy. Although this introduces a risk of selection bias, it is a well established practice,7,29 and we deemed it unethical not to provide patients undergoing a more painful thoracotomy procedure5,30 with an active epidural catheter. Second, the exclusion of trial patients by the surgeon on the grounds of not opting for epidural analgesia introduces a possible selection bias. We speculate, however, that it would have been the less extensive thoracic surgery that would not have had a supplementary epidural catheter inserted. However, the randomisation would still ensure valid and unbiased results if we examine pain in VATS as a whole and not stratify on the type of surgery thought possibly with a diminished treatment effect. Finally, the proportion of missing values related to our study's primary outcome measure of pain was 17% (data not shown). This number should preferably be lower but is comparable to what is generally seen in RCTs31 and other clinical studies using pain scores with missing values ranging from 4 to 34%.32
Despite the benefits of reduced surgical trauma during minimally invasive thoracoscopic surgery, our study demonstrated that it is still a painful procedure, with an alarmingly high frequency of patients experiencing unacceptable pain when postoperative epidural analgesia was omitted. Serious adverse effects of thoracic epidural analgesia are rare.33 However, due to the potential gravity of the complications, epidural catheters should be justified, and avoided if similar pain relief can be achieved without them. Evidence on the efficacy of alternative loco-regional analgesia techniques for postoperative pain management in VATS, especially the paravertebral block, is rapidly emerging,34,35 and recent recommendations advocate its use over epidural analgesia.8 However, further studies comparing epidural analgesia to other forms of postoperative pain management with emphasis on auxilary areas (e.g. effects on chronic postoperative pain, immunological effects, and its impact on postoperative delirium) are required to establish the best pain management after VATS.
Acknowledgements relating to this articleWe thank the patients for their participation in the trial and the nurses and physicians of both the Department of Cardiothoracic Surgery and the Department of Anaesthesia and Intensive Care Medicine at Odense University Hospital for their assistance in collecting data. Additional thanks go to biostatisticians Signe Bedsted Clemmensen and Ulrich Halekoh for assistance rendered on the statistical analyses. Finally, we would like to thank study nurse Susanne Petersen for all her hard work in all aspects of the trial.
Funding statement: this work was supported by the Danish Cancer Society (award no. R150-A10139), The University of Southern Denmark, The Region of Southern Denmark, Oberstinde Kirsten Jensa la Cours Mindelegat (award no. JSP-25076), and the Department of Anesthesia and Intensive Care Medicine, Odense University Hospital, Denmark.
The funders had no role in the study design, data collection, analysis and interpretation, or report writing.
Conflicts of interest: the authors have no conflicts of interest to declare.
Presentations: none.
This manuscript was handled by Matthias Desmet.
References 1. Gan TJ. Poorly controlled postoperative pain: prevalence, consequences, and prevention. J Pain Res 2017; 10:2287–2298. 2. Behera BK, Puri GD, Ghai B. Patient-controlled epidural analgesia with fentanyl and bupivacaine provides better analgesia than intravenous morphine patient-controlled analgesia for early thoracotomy pain. J Postgrad Med 2008; 54:86–90. 3. Ali M, Winter DC, Hanly AM, et al. Prospective, randomized, controlled trial of thoracic epidural or patient-controlled opiate analgesia on perioperative quality of life. Br J Anaesth 2010; 104:292–297. 4. Richardson J, Cheema S. Thoracic paravertebral nerve block. Br J Anaesth 2006; 96:714–779. 5. Bendixen M, Jorgensen OD, Kronborg C, et al. Postoperative pain and quality of life after lobectomy via video-assisted thoracoscopic surgery or anterolateral thoracotomy for early stage lung cancer: a randomised controlled trial. Lancet Oncol 2016; 17:836–844. 6. Nagahiro I, Andou A, Aoe M, et al. Pulmonary function, postoperative pain, and serum cytokine level after lobectomy: a comparison of VATS and conventional procedure. Ann Thorac Surg 2001; 72:362–365. 7. Holbek BL, Horsleben Petersen R, Kehlet H, Hansen HJ. Fast-track video-assisted thoracoscopic surgery: future challenges. Scand Cardiovasc J 2016; 50:78–82. 8. Feray S, Lubach J, Joshi GP, et al. PROSPECT guidelines for video-assisted thoracoscopic surgery: a systematic review and procedure-specific postoperative pain management recommendations.
留言 (0)