
記住我








Managing the chronic effects of stroke (eg, mobility problems, cognitive impairment, and depression) has become a global health priority because of its enormous burden on health care systems [,]. In Canada, >400,000 people live with the effects of stroke, and by 2038, this number is expected to increase to nearly 700,000 []. To meet the needs of this growing population and address international priorities, self-management support interventions for stroke are of growing interest to researchers and health care professionals. Broadly defined, self-management support is a complex intervention that provides people with knowledge, confidence, and skills to manage their chronic condition []. Self-management support interventions have been shown to improve a variety of health outcomes after stroke, including risk factor control [], functional ability [], participation [], and quality of life []. They have also been recommended in recent clinical practice guidelines []. Unfortunately, however, because of limited health care budgets and unequal access to rehabilitation, few Canadians have the opportunity to participate in self-management support interventions following stroke [,]. Increased access to timely, effective, and low-cost stroke self-management support could be provided through mobile health (mHealth) technology–based (eg, smartphone app–based) interventions.
Despite the growing potential, need, and interest in enhancing stroke self-management support interventions with mHealth, the evidence for its effectiveness remains unclear. In previous reviews of poststroke mHealth interventions, connections were drawn to “self-management support”; however, the concept was never explicitly defined or operationalized [-]. In these previous reviews, self-management support was discussed in a way that suggests that it is a newly emerging concept in the literature on poststroke mHealth interventions. Specifically, in the abstract and introduction of 3 reviews, self-management was framed as a key concept in the rationale for the review [,,]. For example, in 1 review, mHealth for self-management was described as a “new strategy for stroke rehabilitation” []. In the discussion of 2 reviews, improved self-management was highlighted as an important outcome of mHealth use [,]. In the conclusion of 1 review, identifying literature on mHealth interventions to support self-management was stated as the purpose of the study []. Although clearly emphasizing an interest in the concept, without explicit definitions or operationalizations, the literature remains challenging to synthesize and compare, which may lead future reviews to draw incorrect conclusions about intervention effectiveness []. To our knowledge, no review has addressed this lack of conceptual clarity; that is, no review has aimed to map the literature on poststroke mHealth interventions according to well-accepted conceptualizations of self-management support.
ObjectivesTo address this gap in the literature, we conducted a scoping review. This method was selected for its utility in clarifying key concepts in the literature, identifying key characteristics related to a concept, and identifying and analyzing knowledge gaps in an emerging field []. The objectives were to (1) identify and describe the types of poststroke mHealth interventions evaluated using a randomized controlled trial (RCT) design, (2) determine whether (and how) such interventions align with well-accepted conceptualizations (theory [] and taxonomy []) of self-management support, and (3) identify the mHealth functions that facilitate self-management. The purpose of this study was to identify gaps in the literature and recommendations for future research related to mHealth-enhanced stroke self-management support.
Using well-established methods [,], a scoping review was conducted. The protocol was not registered. A critical appraisal of the included studies was not conducted as the aim of this review was to map the breadth and depth of conceptualizations, not to draw conclusions about intervention effectiveness []. The PRISMA-ScR (Preferred Reporting Items for Systematic Reviews and Meta-Analyses extension for Scoping Reviews) checklist is provided in [].
Identifying Relevant StudiesIn consultation with 2 librarians, ANT searched MEDLINE, Embase, PsycINFO, CINAHL, AMED, Scopus, and ProQuest Dissertations and Theses Global 3 times (October 2-3, 2020, February 28, 2022, and July 10, 2023). The second and third searches were conducted to identify new literature published between 2020 and 2022 and between 2022 and 2023. The search terms captured 2 search concepts: stroke and mHealth (see for the full Ovid search strategy).
Selecting StudiesANT, JML-M, NC, CT, VN, JR, and SJ conducted level-1 (title and abstract) and level-2 (full-text) screening in duplicate using Covidence (Veritas Health Innovation). Disagreements were resolved through consensus-based discussion. Studies were included if the article reported original research, the study included human participants with stroke or transient ischemic attack, the study evaluated an mHealth intervention (mHealth defined using 2 definitions: those of the World Health Organization—“[the] medical and public health practice supported by mobile devices, such as mobile phones, patient monitoring devices, personal digital assistants [PDAs], and other wireless devices” []—and Akter et al []—“focusing on any wireless technologies [e.g., Bluetooth, GSM, GPRS/3G, Wi-Fi, WiMAX] to transmit various health-related data content and services through mobile devices, including mobile phones, smartphones, PDAs, laptops and Tablet PCs”), and the study was an RCT. The search was limited to RCTs as a preliminary search identified a large number of studies using an RCT design. In addition, as RCTs are typically regarded as the highest in quality and presumably are the farthest along in the technology development process, their influence on research and practice was thought to be the most significant. Studies were excluded if the sample was mixed (eg, acquired brain injury), the intervention included client (person with stroke)–facing technology or equipment that was not clearly mobile and wireless, the article did not report any outcome measures related to intervention effectiveness, and the article was not written in English.
Charting the DataANT developed the data-charting form in collaboration with DRD and EN. ANT charted the data verbatim and then JML-M, NC, CT, VN, JR, and SJ verified the data. Data were charted from the included articles as well as from supplementary materials and protocol papers when referenced. The data-charting form included study characteristics (eg, study aims and outcome measures), participant characteristics (eg, time since stroke and sex or gender), and intervention characteristics (based on the Template for Intervention Description and Replication checklist []). Visual information related to the intervention characteristics was also charted (eg, screenshots of apps).
Collating, Summarizing, and Reporting the ResultsANT completed the data analysis in collaboration with DRD, EN, RHW, and JIC. Quantitative data were analyzed using descriptive statistics, and qualitative data were analyzed using conventional content analysis (objective 1) and directed content analysis (objectives 2 and 3) []. Directed content analysis for objective 2 was guided by the theory by Lorig and Holman [] and the Practical Reviews in Self-Management Support (PRISMS) taxonomy by Pearce et al [] as they are widely cited, slightly different conceptualizations of self-management support (see [,] for the operational definitions of codes). Directed content analysis for objective 3 was guided by the definition of mHealth functions by Cameron et al [] (“the verbs describing the behavior of the system”), examples from previous research on mHealth functions [-], and dictionary definitions [-] (see [-] for the operational definitions of codes).
A total of 29 studies describing 26 interventions were included (see for the PRISMA [Preferred Reporting Items for Systematic Reviews and Meta-Analyses] flow diagram []). The studies were published between 2007 and 2023 and were from Asia (13/29, 45%), Europe (8/29, 28%), North America (4/29, 14%), Africa (2/29, 7%), and Australia (2/29, 7%). Of the 29 studies, 1 (3%) was a doctoral dissertation [] and the remaining 28 (97%) were peer-reviewed journal articles. A total of 34% (10/29) of the studies were considered pilot, proof-of-concept, or feasibility studies. The sample sizes ranged from 11 to 4298. presents the study and participant characteristics.
 Figure 1. PRISMA (Preferred Reporting Items for Systematic Reviews and Meta-Analyses) flow diagram. Table 1. Study and participant characteristics.StudyCountryStudy aimsOutcome measuresSample sizeStroke typeTime since stroke or stroke stageAge (y)Sex or gender (male or men; %)Asano et al []SingaporeEffectivenessLate-Life Function and Disability Instrument; timed 5-Meter Walk Test; 2-minute walk test; Modified Barthel Index; Activities-Specific Balance Confidence Scale; EQ-5D98 (IGa: 50; CGb: 48)78% ischemic; 22% hemorrhagicWithin 4 wkMean 64.1 (range 40.5-89.6)52Emmerson et al []AustraliaEffectivenessSelf-report logbook; Wolf Motor Function Test; customized questionnaire58 (IG: 28; CG: 30)86% ischemic; 15% hemorrhagicMedian 120 (range 58-226) dMean 66 (SD 16)63Ferrete Ruíz et al []SpainEffectivenessMississippi Aphasia Screening Test; minutes of device use30 (IG: 23; CG: 7)100% ischemicWithin 7 dIG: mean 73.20 (SD 9.53); CG: mean 72.40 (SD 2.79)50Grau-Pellicer et al []SpainEffectivenessParticipant reports of community ambulation and sedentary behavior; 10-Meter Walk Test; 6-Minute Walk Test; Timed Up and Go test; Barthel Index; EQ-5D; satisfaction questionnaire34 (IG: 21; CG: 13)Not reportedIG: mean 18.92 (SD 27.6; range 1-96) mo; CG: mean 20.85 (SD 59.74; range 1-252) moIG: mean 62.96 (SD 11.87; range 33-89); CG: mean 68.53 (SD 11.53; range 41-83)51Hankinson et al []AustraliaPilot study; feasibility; effectivenessAdherence to intervention; Fugl-Meyer Assessment15 (IG: 6; CG: 9)Not reported0-180 dNot reported59Ifejika et al []United StatesPilot; feasibility; preliminary effectivenessReduction in total body weight; compliance with the weight loss intervention; Patient Health Questionnaire–9; systolic blood pressure; serum low-density lipoprotein value; proportion of total hemoglobin; proportion of serum coagulation factor VIII25 (IG: 13; CG: 12)Not reportedAcutely hospitalizedMean 54.1 (SD 9.4)56Jang and Jang []South KoreaEffectivenessManual Muscle Test; Manual Function Test; Purdue Pegboard Test21 (IG: 10; CG: 11)19% ischemic; 81% hemorrhagicMean 963 (SD 799) dMean 44.5 (SD 16.5)71Kamal et al []PakistanEffectivenessMorisky Medication Adherence Scale; systolic and diastolic blood pressure; satisfaction questionnaires162 (IG: 83; CG: 79)84% ischemic; 17% hemorrhagicIG: median 2 (range 1-5) mo; CG: median 2 (range 1-4) moIG: mean 56.07 (SD 1.5); CG: mean 57.62 (SD 1.3)68Kamal et al []PakistanEffectiveness; safetySystolic and diastolic blood pressure; blood sugar (HbA1cc); blood cholesterol (low-density lipoprotein level); mortality; modified Rankin Scale; National Institutes of Health Stroke Scale; Barthel Index277 (IG: 141; CG: 136)Not reportedNot reportedIG: mean 60.6 (SD 12); CG: mean 59.7 (SD 14.3)67Kamwesiga et al []SwedenFeasibility study; preliminary effectivenessLogbook to record adherence; Canadian Occupational Performance Measure; self-efficacy scale; Stroke Impact Scale 3.0 Uganda version; Barthel Index; Occupational Gaps Questionnaire, Ugandan version28 (IG: 13; CG: 15)75% ischemic; 21% hemorrhagic; 4% unspecified3-6 mo—IG: 10 (76.9%) and CG: 10 (66.7%); 7-11 mo—IG: 3 (23.1%) and CG: 3 (20%); 1-2 y—IG: 0 and CG: 2 (13.3%)IG: mean 61.2 (SD 15); CG: mean 58.5 (SD 14)25Kang et al []South KoreaEffectivenessRegional House-Brackmann Facial Nerve Grading System; length between the corner of the mouth and the earlobe21 (IG: 10; CG: 11)95% ischemic; 5% hemorrhagicWithin 12 wkIG: mean 63.1 (SD 10.3); CG: mean 55.6 (SD 16)62Kang et al []TaiwanEffectivenessStroke knowledge questionnaire; EQ-5D63 (IG: 30; CG: 33)43% ischemic; 57% hemorrhagicNot reportedIG: mean 50.47 (SD 10.82); CG: mean 52.33 (SD 11.03)68Kenny et al []United KingdomFeasibility; acceptability; preliminary effectivenessMotor Status Scale; Leeds Movement Performance Index; General Self-Efficacy Scale; diary to record time spent exercising11 (IG: 5; CG: 6)77% ischemic; 8% hemorrhagic; 15% unspecifiedNot reportedMean 73.46 (range 41-88)46Kim et al []South KoreaEffectivenessActivities-Specific Balance Confidence Scale; Dynamic Gait Index; Four Square Step Test; Functional Ambulation Categories; Timed Up and Go test; up-stair and down-stair times; spatiotemporal parameters of gait (velocity and cadence)18 (IG: 9; CG: 9)40% ischemic; 60% hemorrhagicIG: mean 5.68 (SD 1.04) mo; CG: mean 4.76 (SD 2.65) moIG: mean 58.3 (SD 11.8); CG: mean 51.8 (SD 13.7)65Labovitz et al []United StatesEffectivenessPill count; plasma sampling; data from artificial intelligence platform27 (IG: 15; CG: 12)100% ischemicNot reportedMean 57 (SD 13.17); median 59 (range 30-79)46Lakshminarayan et al []United StatesPilot, proof-of-concept study; feasibility; usability; acceptability; preliminary effectivenessNumber of days blood pressure data were transmitted; systolic blood pressure; Morisky Medication Adherence Scale50 (IG: 28; CG: 22)Not reportedAcuteIG: mean 63.1 (SD 9.7; range 42-81); CG: mean 68.3 (SD 10.0; range 46-85); withdrawn: mean 60.33 (SD 13.7; range 47-84)68Maresca et al []ItalyPilot study; effectivenessToken Test; Esame Neuropsicologico Per l’Afasia; Aphasic Depression Rating Scale; EQ-5D; Psychosocial Impact of Assistive Devices Scale30 (IG: 15; CG: 15)63% ischemic; 37% hemorrhagicNot reportedMean 51.2 (SD 11.3)47Moon et al []South KoreaEffectivenessFunctional Dysphagia Scale; penetration-aspiration scale; visual analog satisfaction scale16 (IG: 8; CG: 8)88% ischemic; 13% hemorrhagicIG: mean 22.75 (SD 9.21) d; CG: mean 21 (SD 9.02) dIG: mean 54.13 (SD 5.41); CG: mean 55.38 (SD 14.88)56Øra et al []NorwayPilot study; preliminary effectivenessNorwegian Basic Aphasia Assessment; Verb and Sentence Test; Communicative Effectiveness Index62 (IG: 32; CG: 30)69% ischemic; 18% hemorrhagic; 13% both≤3 mo—IG: 16 (50%) and CG: 12 (40%); 3-12 mo—IG: 5 (15.6%) and CG: 4 (13.3%); >12 mo—IG: 11 (34.4%) and CG: 14 (46.7%)IG: mean 64.7 (SD 11.7); CG: mean 65 (SD 12.2)66Pandian et al []IndiaEffectivenessComposite end point of recurrent stroke, high-risk transient ischemic attack, acute coronary syndrome, and all-cause mortality; change in BMI; physical activity total metabolic equivalent (min/wk); current smoking; current alcohol intake; modified Rankin Scale; medication noncompliance; systolic and diastolic blood pressure (mm Hg); fasting blood sugar (mg/dL); low-density lipoprotein cholesterol (mg/dL); triglycerides (mg/dL)4298 (IG: 2148; CG: 2150)83% ischemic; 17% hemorrhagic2 d to 3 moIG: median 56 (range 18-88); CG: median 56 (range 18-89)73Radomski []United StatesEffectivenessEveryday habit questionnaire; self-reported adherence to self-care checklist; Functional Independence Measure; Frenchay Activities Index; Caregiver’s Burden Scale; performance time for self-care task (seconds)15 (IG: 5; CG 1: 5; CG 2: 5)Not reportedNot reportedMean 59 (SD 14)80Sarfo et al []GhanaPilot; feasibility; preliminary effectivenessSystolic and diastolic blood pressure; medication possession ratio; perceived confidence scale; Treatment Self-Regulation Questionnaire56 (IG: 29; CG: 27)77% ischemic; 23% hemorrhagic<1 moIG: mean 54.3 (SD 11.9); CG: mean 55.9 (SD 13.7)65Sarfo et al []GhanaPilot study; preliminary effectivenessSystolic and diastolic blood pressure; medication possession ratio score; Morisky Medication Adherence Scale; perceived confidence scale; Treatment Self-Regulation Questionnaire; Telemedicine Satisfaction and Usefulness Questionnaire; hypertension and stroke knowledge 14-item questionnaire55 (IG: 28; CG: 27)77% ischemic; 23% hemorrhagic<1 moIG: mean 54.3 (SD 11.9); CG: mean 55.9 (SD 13.7)65Tomori et al []JapanPilot study; feasibility; preliminary effectiveness36-Item Short Form Health Survey; Brunnstrom recovery stages; Functional Independence Measure; Client Satisfaction Questionnaire; duration of stay37 (IG: 16; CG: 21)Not reported≥30 d; subacuteMean 66.22 (SD 10.64)67Vahlberg et al []SwedenEffectiveness6-Minute Walk Test (m); chair stand test (s); 10-Meter Walk Test (m/s); Short Physical Performance Battery79 (IG: 40; CG: 39)72% ischemic; 11% hemorrhagic; 17% transient ischemic attackMean 6 (SD 4.4) dIG: mean 63.9 (SD 10.1); CG: mean 63.9 (SD 10.8)63Vahlberg et al []SwedenEffectivenessFat-free mass (kg); fat mass (kg); BMI; body weight (kg); HbA1c; serum insulin-like growth factor; low- and high-density lipoprotein cholesterol; self-reported health; mortality71 (IG: 36; CG: 35)72% ischemic; 11% hemorrhagic; 17% transient ischemic attackMedian 5 dIG: mean 63.9 (SD 10); CG: mean 63.9 (SD 10)63Wan et al []ChinaEffectivenessSystolic and diastolic blood pressure; Health-Promoting Lifestyle Profile II158 (IG: 80; CG: 78)100% ischemicWithin 1 moMedian 63.8165Wang et al []ChinaEffectivenessHealth-Promoting Lifestyle Profile II; systolic and diastolic blood pressure; modified Rankin Scale; stroke recurrence151 (IG: 76; CG: 75)100% ischemicWithin 1 moMedian 63.8066Wang et al []ChinaEffectivenessSystolic blood pressure; Self-Management Ability Scale; Morisky Medication Adherence Scale; BMI; blood low-density lipoprotein193 (IG: 98; CG: 95)67% ischemic; 33% hemorrhagicNot reportedIG: mean 42.75 (SD 0.16); CG: mean 41.32 (SD 2.16)61
Figure 1. PRISMA (Preferred Reporting Items for Systematic Reviews and Meta-Analyses) flow diagram. Table 1. Study and participant characteristics.StudyCountryStudy aimsOutcome measuresSample sizeStroke typeTime since stroke or stroke stageAge (y)Sex or gender (male or men; %)Asano et al []SingaporeEffectivenessLate-Life Function and Disability Instrument; timed 5-Meter Walk Test; 2-minute walk test; Modified Barthel Index; Activities-Specific Balance Confidence Scale; EQ-5D98 (IGa: 50; CGb: 48)78% ischemic; 22% hemorrhagicWithin 4 wkMean 64.1 (range 40.5-89.6)52Emmerson et al []AustraliaEffectivenessSelf-report logbook; Wolf Motor Function Test; customized questionnaire58 (IG: 28; CG: 30)86% ischemic; 15% hemorrhagicMedian 120 (range 58-226) dMean 66 (SD 16)63Ferrete Ruíz et al []SpainEffectivenessMississippi Aphasia Screening Test; minutes of device use30 (IG: 23; CG: 7)100% ischemicWithin 7 dIG: mean 73.20 (SD 9.53); CG: mean 72.40 (SD 2.79)50Grau-Pellicer et al []SpainEffectivenessParticipant reports of community ambulation and sedentary behavior; 10-Meter Walk Test; 6-Minute Walk Test; Timed Up and Go test; Barthel Index; EQ-5D; satisfaction questionnaire34 (IG: 21; CG: 13)Not reportedIG: mean 18.92 (SD 27.6; range 1-96) mo; CG: mean 20.85 (SD 59.74; range 1-252) moIG: mean 62.96 (SD 11.87; range 33-89); CG: mean 68.53 (SD 11.53; range 41-83)51Hankinson et al []AustraliaPilot study; feasibility; effectivenessAdherence to intervention; Fugl-Meyer Assessment15 (IG: 6; CG: 9)Not reported0-180 dNot reported59Ifejika et al []United StatesPilot; feasibility; preliminary effectivenessReduction in total body weight; compliance with the weight loss intervention; Patient Health Questionnaire–9; systolic blood pressure; serum low-density lipoprotein value; proportion of total hemoglobin; proportion of serum coagulation factor VIII25 (IG: 13; CG: 12)Not reportedAcutely hospitalizedMean 54.1 (SD 9.4)56Jang and Jang []South KoreaEffectivenessManual Muscle Test; Manual Function Test; Purdue Pegboard Test21 (IG: 10; CG: 11)19% ischemic; 81% hemorrhagicMean 963 (SD 799) dMean 44.5 (SD 16.5)71Kamal et al []PakistanEffectivenessMorisky Medication Adherence Scale; systolic and diastolic blood pressure; satisfaction questionnaires162 (IG: 83; CG: 79)84% ischemic; 17% hemorrhagicIG: median 2 (range 1-5) mo; CG: median 2 (range 1-4) moIG: mean 56.07 (SD 1.5); CG: mean 57.62 (SD 1.3)68Kamal et al []PakistanEffectiveness; safetySystolic and diastolic blood pressure; blood sugar (HbA1cc); blood cholesterol (low-density lipoprotein level); mortality; modified Rankin Scale; National Institutes of Health Stroke Scale; Barthel Index277 (IG: 141; CG: 136)Not reportedNot reportedIG: mean 60.6 (SD 12); CG: mean 59.7 (SD 14.3)67Kamwesiga et al []SwedenFeasibility study; preliminary effectivenessLogbook to record adherence; Canadian Occupational Performance Measure; self-efficacy scale; Stroke Impact Scale 3.0 Uganda version; Barthel Index; Occupational Gaps Questionnaire, Ugandan version28 (IG: 13; CG: 15)75% ischemic; 21% hemorrhagic; 4% unspecified3-6 mo—IG: 10 (76.9%) and CG: 10 (66.7%); 7-11 mo—IG: 3 (23.1%) and CG: 3 (20%); 1-2 y—IG: 0 and CG: 2 (13.3%)IG: mean 61.2 (SD 15); CG: mean 58.5 (SD 14)25Kang et al []South KoreaEffectivenessRegional House-Brackmann Facial Nerve Grading System; length between the corner of the mouth and the earlobe21 (IG: 10; CG: 11)95% ischemic; 5% hemorrhagicWithin 12 wkIG: mean 63.1 (SD 10.3); CG: mean 55.6 (SD 16)62Kang et al []TaiwanEffectivenessStroke knowledge questionnaire; EQ-5D63 (IG: 30; CG: 33)43% ischemic; 57% hemorrhagicNot reportedIG: mean 50.47 (SD 10.82); CG: mean 52.33 (SD 11.03)68Kenny et al []United KingdomFeasibility; acceptability; preliminary effectivenessMotor Status Scale; Leeds Movement Performance Index; General Self-Efficacy Scale; diary to record time spent exercising11 (IG: 5; CG: 6)77% ischemic; 8% hemorrhagic; 15% unspecifiedNot reportedMean 73.46 (range 41-88)46Kim et al []South KoreaEffectivenessActivities-Specific Balance Confidence Scale; Dynamic Gait Index; Four Square Step Test; Functional Ambulation Categories; Timed Up and Go test; up-stair and down-stair times; spatiotemporal parameters of gait (velocity and cadence)18 (IG: 9; CG: 9)40% ischemic; 60% hemorrhagicIG: mean 5.68 (SD 1.04) mo; CG: mean 4.76 (SD 2.65) moIG: mean 58.3 (SD 11.8); CG: mean 51.8 (SD 13.7)65Labovitz et al []United StatesEffectivenessPill count; plasma sampling; data from artificial intelligence platform27 (IG: 15; CG: 12)100% ischemicNot reportedMean 57 (SD 13.17); median 59 (range 30-79)46Lakshminarayan et al []United StatesPilot, proof-of-concept study; feasibility; usability; acceptability; preliminary effectivenessNumber of days blood pressure data were transmitted; systolic blood pressure; Morisky Medication Adherence Scale50 (IG: 28; CG: 22)Not reportedAcuteIG: mean 63.1 (SD 9.7; range 42-81); CG: mean 68.3 (SD 10.0; range 46-85); withdrawn: mean 60.33 (SD 13.7; range 47-84)68Maresca et al []ItalyPilot study; effectivenessToken Test; Esame Neuropsicologico Per l’Afasia; Aphasic Depression Rating Scale; EQ-5D; Psychosocial Impact of Assistive Devices Scale30 (IG: 15; CG: 15)63% ischemic; 37% hemorrhagicNot reportedMean 51.2 (SD 11.3)47Moon et al []South KoreaEffectivenessFunctional Dysphagia Scale; penetration-aspiration scale; visual analog satisfaction scale16 (IG: 8; CG: 8)88% ischemic; 13% hemorrhagicIG: mean 22.75 (SD 9.21) d; CG: mean 21 (SD 9.02) dIG: mean 54.13 (SD 5.41); CG: mean 55.38 (SD 14.88)56Øra et al []NorwayPilot study; preliminary effectivenessNorwegian Basic Aphasia Assessment; Verb and Sentence Test; Communicative Effectiveness Index62 (IG: 32; CG: 30)69% ischemic; 18% hemorrhagic; 13% both≤3 mo—IG: 16 (50%) and CG: 12 (40%); 3-12 mo—IG: 5 (15.6%) and CG: 4 (13.3%); >12 mo—IG: 11 (34.4%) and CG: 14 (46.7%)IG: mean 64.7 (SD 11.7); CG: mean 65 (SD 12.2)66Pandian et al []IndiaEffectivenessComposite end point of recurrent stroke, high-risk transient ischemic attack, acute coronary syndrome, and all-cause mortality; change in BMI; physical activity total metabolic equivalent (min/wk); current smoking; current alcohol intake; modified Rankin Scale; medication noncompliance; systolic and diastolic blood pressure (mm Hg); fasting blood sugar (mg/dL); low-density lipoprotein cholesterol (mg/dL); triglycerides (mg/dL)4298 (IG: 2148; CG: 2150)83% ischemic; 17% hemorrhagic2 d to 3 moIG: median 56 (range 18-88); CG: median 56 (range 18-89)73Radomski []United StatesEffectivenessEveryday habit questionnaire; self-reported adherence to self-care checklist; Functional Independence Measure; Frenchay Activities Index; Caregiver’s Burden Scale; performance time for self-care task (seconds)15 (IG: 5; CG 1: 5; CG 2: 5)Not reportedNot reportedMean 59 (SD 14)80Sarfo et al []GhanaPilot; feasibility; preliminary effectivenessSystolic and diastolic blood pressure; medication possession ratio; perceived confidence scale; Treatment Self-Regulation Questionnaire56 (IG: 29; CG: 27)77% ischemic; 23% hemorrhagic<1 moIG: mean 54.3 (SD 11.9); CG: mean 55.9 (SD 13.7)65Sarfo et al []GhanaPilot study; preliminary effectivenessSystolic and diastolic blood pressure; medication possession ratio score; Morisky Medication Adherence Scale; perceived confidence scale; Treatment Self-Regulation Questionnaire; Telemedicine Satisfaction and Usefulness Questionnaire; hypertension and stroke knowledge 14-item questionnaire55 (IG: 28; CG: 27)77% ischemic; 23% hemorrhagic<1 moIG: mean 54.3 (SD 11.9); CG: mean 55.9 (SD 13.7)65Tomori et al []JapanPilot study; feasibility; preliminary effectiveness36-Item Short Form Health Survey; Brunnstrom recovery stages; Functional Independence Measure; Client Satisfaction Questionnaire; duration of stay37 (IG: 16; CG: 21)Not reported≥30 d; subacuteMean 66.22 (SD 10.64)67Vahlberg et al []SwedenEffectiveness6-Minute Walk Test (m); chair stand test (s); 10-Meter Walk Test (m/s); Short Physical Performance Battery79 (IG: 40; CG: 39)72% ischemic; 11% hemorrhagic; 17% transient ischemic attackMean 6 (SD 4.4) dIG: mean 63.9 (SD 10.1); CG: mean 63.9 (SD 10.8)63Vahlberg et al []SwedenEffectivenessFat-free mass (kg); fat mass (kg); BMI; body weight (kg); HbA1c; serum insulin-like growth factor; low- and high-density lipoprotein cholesterol; self-reported health; mortality71 (IG: 36; CG: 35)72% ischemic; 11% hemorrhagic; 17% transient ischemic attackMedian 5 dIG: mean 63.9 (SD 10); CG: mean 63.9 (SD 10)63Wan et al []ChinaEffectivenessSystolic and diastolic blood pressure; Health-Promoting Lifestyle Profile II158 (IG: 80; CG: 78)100% ischemicWithin 1 moMedian 63.8165Wang et al []ChinaEffectivenessHealth-Promoting Lifestyle Profile II; systolic and diastolic blood pressure; modified Rankin Scale; stroke recurrence151 (IG: 76; CG: 75)100% ischemicWithin 1 moMedian 63.8066Wang et al []ChinaEffectivenessSystolic blood pressure; Self-Management Ability Scale; Morisky Medication Adherence Scale; BMI; blood low-density lipoprotein193 (IG: 98; CG: 95)67% ischemic; 33% hemorrhagicNot reportedIG: mean 42.75 (SD 0.16); CG: mean 41.32 (SD 2.16)61aIG: intervention group.
bCG: control group.
cHbA1c: glycated hemoglobin.
Participant CharacteristicsIn total, 62% (18/29) of the studies included participants with both ischemic and hemorrhagic stroke, and 7% (2/29) also included transient ischemic attack. Of the 23 studies that reported participants’ stroke stage or time since stroke, 16 (70%) focused on the subacute stage (7 d to 6 mo after stroke). The average age of the participants ranged from 42 to 74 years (weighted average 57, weighted SD 4.46). No studies differentiated between sex and gender. A total of 83% (24/29) of the studies included more male participants or men than female participants or women, ranging from 25% to 80% of male participants or men. Some studies reported on participants’ education (15/29, 52%), marital status (8/29, 28%), employment status (6/29, 21%), and geographic location (5/29, 17%), and fewer studies reported on race (3/29, 10%), ethnicity (1/29, 3%), and income (2/29, 7%).
Objective 1: Types of Poststroke mHealth Interventions[-] summarizes the interventions individually and the following sections summarize the interventions collectively, according to selected items from the Template for Intervention Description and Replication checklist [].
Why: Describe Any Rationale, Theory, or Goal of the Elements Essential to the InterventionmHealth technology was rationalized as a strategy to improve intervention effectiveness (18/26, 69%), access (13/26, 50%), convenience (6/26, 23%), and cost-effectiveness (5/26, 19%). A total of 5 interventions were explicitly based on a theory, model, framework, or taxonomy: self-determination theory (n=2, 40%); Health Belief Model (n=2, 40%); social cognitive theory (n=1, 20%); the International Classification of Functioning, Disability, and Health framework (n=1, 20%); the Coventry, Aberdeen, and London–Refined taxonomy of behavior change techniques (n=1, 20%); and a proposed ecological model of adherence to rehabilitation treatment recommendations (n=1, 20%). Common goals of the interventions were to improve outcomes related to treatment or medication adherence (10/26, 38%), motor or physical activity (8/26, 31%), functional ability or independence (5/26, 19%), speech, language, or swallowing (5/26, 19%), hypertension or blood pressure control (5/26, 19%), risk factor control (5/26, 19%), and quality of life (3/26, 12%).
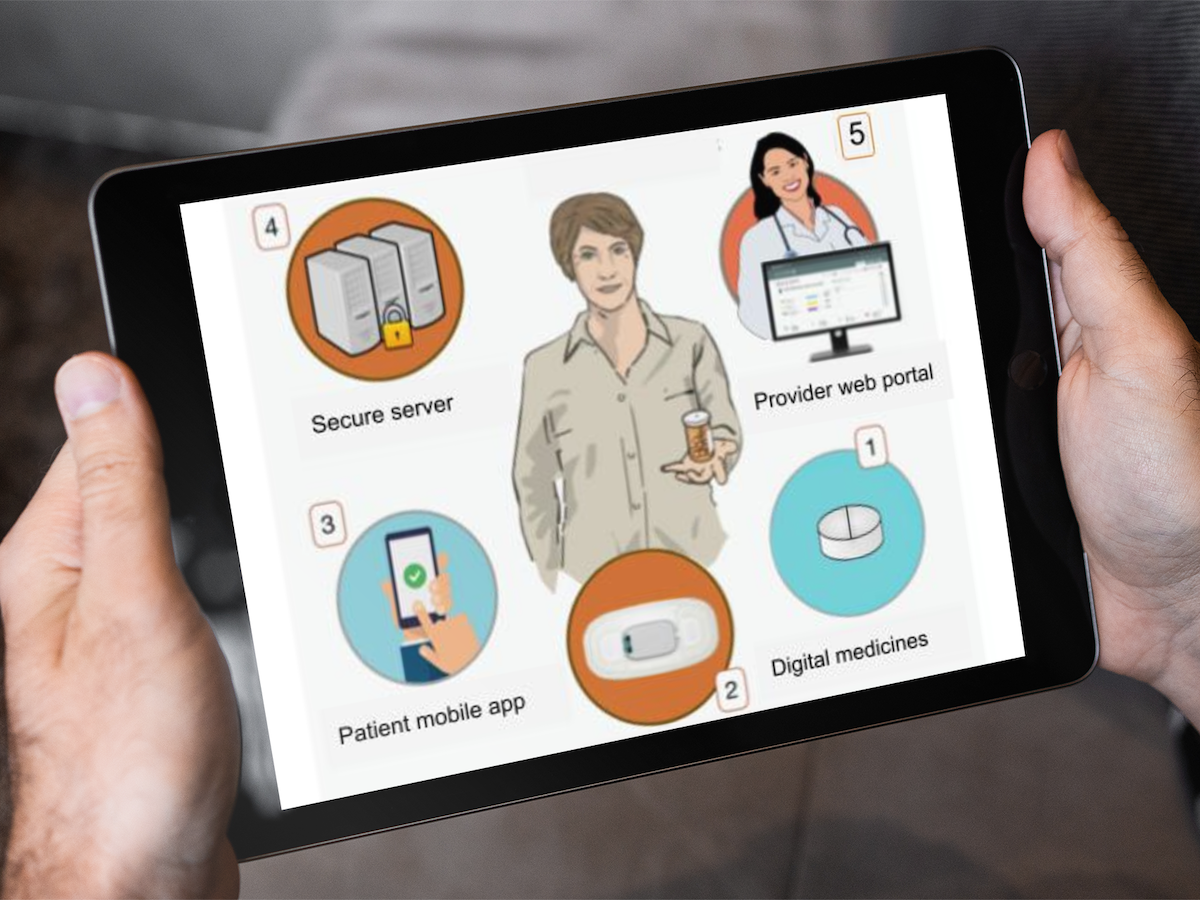
What: Describe Any Physical or Informational Materials Used and Each of the Procedures, Activities, or Processes Used in the InterventionA total of 7 focal areas were identified: physical exercise (10/26, 38%), risk factor management (5/26, 19%), linguistic exercise (3/26, 12%), activities of daily living (ADLs) training (3/26, 12%), medication adherence (2/26, 8%), stroke education (2/26, 8%), and weight management (1/26, 4%). In total, 5 types of mobile devices were used: mobile phones or smartphones (17/26, 65%), tablets (9/26, 35%), wearable sensors (5/26, 19%; eg, pedometers or wearable bracelets), wireless monitoring devices (4/26, 15%; eg, Bluetooth sphygmomanometers or Bluetooth blood glucose meters), and laptops (1/26, 4%). Within devices, the features used included: apps (15/26, 58%), messaging (12/26, 46%; eg, via an app or SMS text messaging), phone calling (7/26, 27%), videos (6/26, 23%), videoconferencing (3/26, 12%), and email (2/26, 8%). All but 4 interventions (22/26, 85%) were self-directed, and 8% (2/26) were gamified.
Who Provided: For Each Category of Intervention Provider, Describe Their BackgroundThe interventions were provided by researchers (9/26, 35%), occupational therapists (7/26, 27%), physical therapists (4/26, 15%), nurses (4/26, 15%), speech-language pathologists (2/26, 8%), physicians (2/26, 8%), pharmacists (1/26, 4%), neuropsychologists (1/26, 4%), brain and heart health managers (1/26, 4%), allied health professionals (1/26, 4%), clinicians (1/26, 4%), and clinic staff (1/26, 4%). In total, 12% (3/26) were provided by a multidisciplinary team of health care professionals.
How: Describe the Modes of Delivery of the Intervention and Whether It Was Provided Individually or in a GroupA total of 85% (22/26) of the interventions were delivered both virtually (eg, via videoconferencing or SMS text messaging) and in-person (eg, in-person orientation or clinic visits). In total, 77% (20/26) were individual based (delivered to the individual with stroke), 38% (10/26) were dyad based (delivered to the individual with stroke and their caregiver or family member), and 8% (2/26) were group based (delivered to groups of people with stroke).
Where: Describe the Types of Locations Where the Intervention OccurredIn total, 58% (15/26) of the interventions occurred both at the hospital or clinic (in-person component) and the participants’ home (virtual component).
When and How Much: Describe the Number of Times the Intervention Was Delivered and Over What PeriodIntervention delivery time ranged from 14 days to 1 year, with the most common being 4 weeks (5/26, 19%) and 6 months (5/26, 19%). Session frequency varied (twice/d to once every 2-3 mo), as did session length (5 min to 1 h). This variability reflects a wide range of session types (eg, exercise sessions, education sessions, blood pressure self-monitoring, and clinic visits). There was also variability in the dosage of technology used, such as the schedule for sending and receiving messages (twice/d to once/wk) and the amount of time connected to the devices (eg, 1 intervention required participants to wear a pedometer at all times except when sleeping, bathing, or swimming).
Tailoring: If the Intervention Was Planned to be Personalized, Titrated, or Adapted, Describe What, Why, When, and HowA total of 69% (18/26) of the interventions involved tailoring to the person with stroke (eg, abilities, goals, or preferred music). In total, 8% (2/26) of the interventions involved tailoring to the caregiver or family member (eg, preferred ADLs) [,]. A total of 12% (3/26) of the interventions involved self-tailoring by the person with stroke (eg, education topics [] or exercises [,,]).
Objective 2: Alignment With Self-Management Support Theory and TaxonomyOf the 29 conceptual variables, 26 (90%) were coded at least once. The number of interventions coded per variable ranged from 0 to 25 (mean 8.55). The number of variables coded per intervention ranged from 2 to 15 (mean 9.54). [,,-] presents the extent and range of alignment, and presents the nature of alignment.
 Figure 2. Extent and range of alignment between poststroke mobile technology–based interventions and self-management support theory and taxonomy. Please see for a larger version. Table 2. Nature of alignment between poststroke mobile technology–based interventions and self-management support theory and taxonomy.Conceptual variableIntervention examplesSelf-management support theory []
Figure 2. Extent and range of alignment between poststroke mobile technology–based interventions and self-management support theory and taxonomy. Please see for a larger version. Table 2. Nature of alignment between poststroke mobile technology–based interventions and self-management support theory and taxonomy.Conceptual variableIntervention examplesSelf-management support theory []aADL: activity of daily living.
Objective 3: mHealth Functions That Facilitate Self-ManagementAcross all conceptual variables and interventions, 7 mHealth functions were identified as facilitating self-management: educating, communicating, goal setting, monitoring, providing feedback, reminding, and motivating.
To our knowledge, this is the first scoping review to map the literature on poststroke mHealth interventions according to a self-management support theory and taxonomy. A total of 29 studies describing 26 interventions were included. Overall, we found that the interventions addressed 7 focal areas, 5 types of mobile devices, and 7 mHealth functions. Collectively, the interventions aligned well with the concept of self-management support. However, on an individual basis (per intervention), the alignment was less strong. The following sections further explain how this review extends previous reviews on poststroke mHealth [-,-] and telehealth [] interventions in relation to the study objectives and interventions included.
Objective 1: Types of Poststroke mHealth InterventionsFocal Areas: Current Trends and GapsOur first objective was to identify and describe the types of poststroke mHealth interventions evaluated using an RCT design. Speaking to such types, 7 focal areas were identified: physical exercise, risk factor management, linguistic exercise, ADLs training, medication adherence, stroke education, and weight management. These 7 focal areas have been identified in previous reviews on poststroke mHealth interventions [-,-]; however, the included interventions varied. Compared with previous reviews, 45% (13/29) of the studies included in our review (12 interventions) had not been previously identified. Similar to previous reviews, this review found the most common focal area to be physical exercise, likely reflecting the rising trend within the general population of using mobile technology to promote physical fitness in everyday life [,]. Hence, the literature clearly supports continued research on poststroke mHealth interventions for physical exercise. Also consistent with previous reviews, this review did not identify any interventions focused on mood or fatigue. Considering the high prevalence of poststroke depression, anxiety, and fatigue, this is a serious gap that should be addressed in future research []. Surprisingly, unlike 5 previous reviews [,,,,], this review did not identify any interventions focused on cognition. This difference was due to the varying eligibility criteria (eg, study design). Given this difference across reviews as well as the high prevalence of poststroke cognitive impairment [], future research on poststroke mHealth interventions for cognition is encouraged to progress toward the level of RCTs.
mHealth Technology: Positioning on the Spectrum of DefinitionsRegarding the types of technology used in the interventions, our review identified 5 types of mobile devices (mobile phones or smartphones, tablets, wearable sensors, wireless monitoring devices, and laptops) and 6 features within these devices (apps, messaging, phone calling, videos, videoconferencing, and email). This wide range of technologies resulted from our novel approach to defining mHealth. Previous reviews on poststroke mHealth interventions have defined mHealth either very narrowly, focusing on a few specific mobile devices or features (eg, mobile phones [], wearable activity monitors [], or mobile apps for phones [,,,,] and tablets [,,,,]), or very broadly, focusing on mHealth in general and including devices and features that may not be entirely mobile and wireless (eg, computer programs [,,], telephone calls [], and web-based applications []). Our review was interested in the literature between these 2 ends of the narrow-broad spectrum of mHealth definitions. We followed the recommendation of Cameron et al [] to define mHealth in a way that captures the “combinatorial complexity” of the mobile system and used 2 open-ended definitions of mHealth [,]. Thus, we captured additional literature on poststroke mHealth interventions by focusing on entirely mobile systems (technology and equipment) of any type (devices and features). As the field of mHealth continues to grow, we suggest that future reviews explicitly position themselves on this narrow-broad spectrum of mHealth definitions so that the literature can be more readily interpreted and applied. In addition, future work should build on that by Cameron et al [] to further deepen our understanding of the mobile system.
Objective 2: Alignment With Self-Management Support Theory and TaxonomyOur second objective was to determine whether (and how) the included interventions aligned with well-accepted conceptualizations (theory [] and taxonomy []) of self-management support. Collectively, the interventions addressed 90% (26/29) of the conceptual variables, whereas individual interventions only addressed an average of 33% (9.54/29) of the conceptual variables. This discrepancy speaks to the potential for improvements in the alignment between poststroke mHealth interventions and the concept of self-management support. The results also revealed key conceptual variables missing from the literature, such as “emotional self-management” and “information about available resources.” Hence, the results suggest that future research should be more closely aligned with the theory and taxonomy of self-management support. Previous reviews on poststroke mHealth interventions [-,-] have not mapped the literature in this way. However, a review of poststroke telehealth interventions [] used the PRISMS taxonomy [] in a similar way, further validating the relevance of this approach.
Objective 3: mHealth Functions That Facilitate Self-ManagementOur third objective was to identify the mHealth functions that facilitate self-management. A total of 7 mHealth functions were identified: educating, communicating, goal setting, monitoring, providing feedback, reminding, and motivating. These 7 functions, although together framed as facilitating self-management, are not inherently specific to self-management support interventions as they speak generally to what the intervention does, not specifically to what the intervention is about. Viewing mHealth functions in this way, as generic “verbs describing the behavior of the system” [] or as action words that link technology capabilities with intervention components, has not been done in past reviews on poststroke mHealth interventions [-,-]. However, this approach to conceptualizing mHealth functions does align with other work in the broader field of mHealth [,]. Future research is encouraged to build on this approach and use the identified functions to describe how specific technology capabilities are linked to specific intervention components. Specifically linking technology capabilities with intervention components is important as it would allow for more systematic examinations as to what it is about delivery through mHealth that may be superior or not to other intervention delivery modalities (eg, is educating on sensitive topics via mHealth better than via in-person groups?).
Recommendations for Future ResearchThe purpose of this study was to identify gaps in the literature and recommendations for future research related to mHealth-enhanced stroke self-management support. In total, 3 overarching recommendations for future research were identified. First, future research should be more explicit about the theories their interventions are based on as well as their conceptualizations of self-management support. Using theory and other conceptualizations in this way would help promote a common language of self-management support and ensure that all conceptual variables are considered, which could ultimately improve intervention adherence, effectiveness, replicability, and uptake in clinical practice. Second, future research should be more multidisciplinary so that a wider range of conceptual variables can be addressed per intervention. This multidisciplinary approach to improving alignment would likely lead to more comprehensive, holistic, and effective interventions. Third, future research should use larger sample sizes and consider using pragmatic trial designs to establish real-world effectiveness.
LimitationsThe search was limited to the English language, so the findings may be biased toward English-speaking countries, although 15 countries were represented. Directed content analysis, as with any qualitative approach, involves subjectivity; to address this, operational definitions for codes were used and reported. Finally, this review focused on RCTs, so the findings may be biased toward more traditional or RCT-suited interventions. Given the challenges associated with conducting RCTs on technology-based interventions [], future reviews should consider including other study designs.
ConclusionsThis scoping review clarified the concept of self-management support in the literature on poststroke mHealth interventions by mapping studies according to well-accepted conceptualizations of self-management support. On the basis of the results, it is recommended that future research on poststroke mHealth interventions be more theoretically driven, more multidisciplinary, and larger in scale.
This research is part of the doctoral work of ANT, which was funded by the Queen Elizabeth II Graduate Scholarship in Science and Technology, Ontario Graduate Scholarship, Ydessa Hendeles Graduate Scholarship at Baycrest Award, and Toronto Rehabilitation Institute Student Scholarship. EN is supported by a Canada Research Chair (Tier 2) in Resiliency and Rehabilitation funded by the Canada Research Chairs Program. The authors gratefully acknowledge Erica Nekolaichuk and Jessica Shiers-Hanley, librarians at the University of Toronto, for their assistance in developing the search strategy.
ANT conceptualized and designed the study under the guidance of DRD and EN. ANT searched the databases. ANT, JML-M, NC, CT, VN, JR, and SJ screened the articles. ANT extracted the data. JML-M, NC, CT, VN, JR, and SJ verified the data. ANT analyzed the data and wrote the manuscript in collaboration with DRD, EN, RHW, and JIC. All authors have reviewed the final manuscript.
None declared.
Edited by L Buis; submitted 16.02.23; peer-reviewed by M Peeples, E Nabovati; comments to author 03.07.23; revised version received 03.10.23; accepted 18.10.23; published 06.12.23
©Alexandra N Thompson, Deirdre R Dawson, Jean Michelle Legasto-Mulvale, Nivetha Chandran, Chelsea Tanchip, Veronika Niemczyk, Jillian Rashkovan, Saisa Jeyakumar, Rosalie H Wang, Jill I Cameron, Emily Nalder. Originally published in JMIR mHealth and uHealth (https://mhealth.jmir.org), 06.12.2023.
This is an open-access article distributed under the terms of the Creative Commons Attribution License (https://creativecommons.org/licenses/by/4.0/), which permits unrestricted use, distribution, and reproduction in any medium, provided the original work, first published in JMIR mHealth and uHealth, is properly cited. The complete bibliographic information, a link to the original publication on https://mhealth.jmir.org/, as well as this copyright and license information must be included.
留言 (0)