
記住我

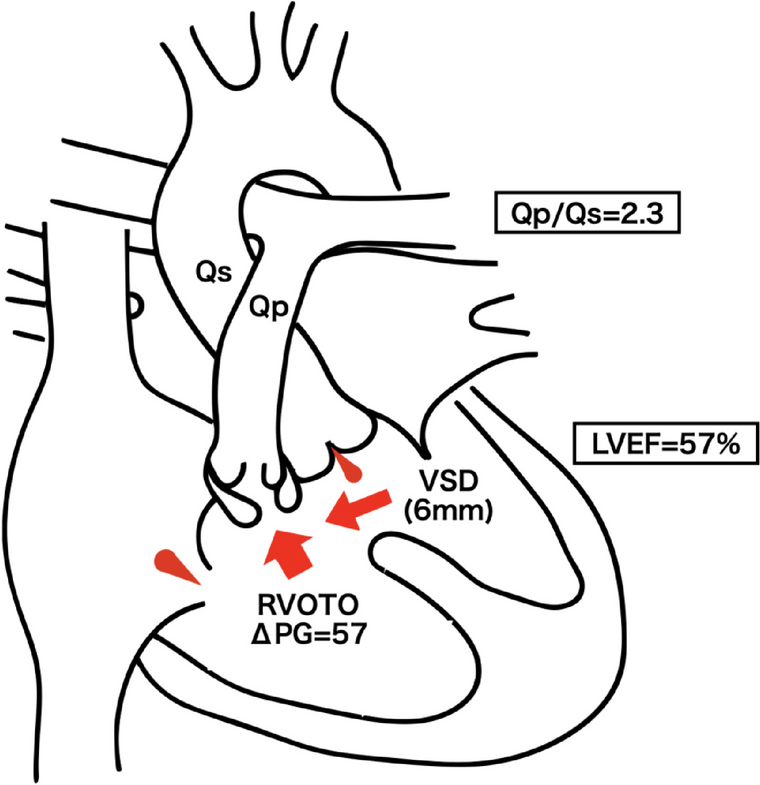


A 41-year-old woman (height 161.0 cm, body weight 45.4 kg) was transferred to our hospital because of acute IE and high fever. Blood cultures were positive for Streptococcus pyogenes. She was diagnosed with TOF accompanied by PA and MAPCAs in childhood. However, no radial surgery was performed because pulmonary blood flow was maintained through the MAPCAs. She was not taking any medications. Transesophageal echocardiography (TEE) performed at a local hospital revealed a 14 mm × 7 mm mobile vegetation attached to the right coronary cusp (Fig. 1), accompanied by moderate aortic regurgitation was also detected. The right ventricular outflow tract was not detected. There were no signs of heart failure. As vegetation gradually increased despite intravenous antibiotic administration, she was scheduled to undergo urgent AVR with CPB.
Fig. 1
Transesophageal echocardiography revealed a 14 × 7 mm mobile vegetation attached to the right coronary cusp (arrowhead). Moderate aortic regurgitation was detected using transesophageal color Doppler imaging. The right ventricular outflow tract was not detected. Ao, aorta; LA, left atrium; LV, left ventricle; RV, right ventricle; VSD, ventricular septal defect
Upon admission, her oxygen saturation was 81% with 2 L/min via nasal cannula. Hemoglobin was elevated at 20.1 mg/dL (normal range: 12–16 mg/dL), and hematocrit was 61.6%. Chest radiography revealed a boot-shaped heart without pulmonary congestion (Fig. 2). Electrocardiography indicated sinus rhythm (heart rate 89/min) and right axis deviation. The 3D computed tomography shows that MAPCAs arise from descending aorta and course to bilateral pulmonary arteries (Fig. 3). Pulmonary blood flow through collateral flow returned directly to the left ventricle, venous drainage from only the SVC and IVC during CPB was predicted to be insufficient for adequate myocardial protection and a bloodless surgical field. Therefore, the intra-aortic balloon occlusion technique of the two main MAPCAs was planned.
Fig. 2
The anteroposterior chest radiography showed a boot-shaped heart and no pulmonary congestion
Fig. 3
The 3D computed tomography shows that major aortopulmonary collateral arteries (MAPCAs) arise from descending aorta and course to bilateral pulmonary arteries. Upper MAPCA (arrow) courses to the left lung and the lower MAPCA (arrowhead) to the right lung
In the operating room, the continuous monitoring included electrocardiogram, SpO2, arterial blood pressure, and arterial pressure-based cardiac output via a left radial artery catheter (FloTrac Sensor; Edwards Lifesciences Corporation, Irvine, CA, USA) before anesthesia induction. At baseline, NIBP was 126/74 mmHg, heart rate 102/min, and SpO2 82% at 2 L/min via a nasal cannula. General anesthesia was induced by intravenous administration of midazolam (4 mg), 0.3 mg fentanyl, and 50 mg rocuronium. After tracheal intubation, a TEE probe was inserted. Additionally, a central venous catheter (PreSep Catheter; Edwards Lifesciences) was inserted via the right internal jugular vein to continuously monitor central venous pressure and oxygen saturation.
Standard median sternotomy was performed under general anesthesia. The superior vena cava (SVC) and inferior vena cava (IVC) were used for venous drainage, and antegrade systemic perfusion was performed via the ascending aorta. As expected preoperatively, venous drainage from only the SVC and IVC was insufficient for adequate myocardial protection and a bloodless surgical field. Intra-aortic balloon via the femoral artery was inflated to block pulmonary blood flow through the two main MAPCAs. Balloon occlusion placement was confirmed using fluoroscopy (Fig. 4) and TEE (Fig. 5). It took about 15 min to place the intra-aortic balloon precisely. During balloon inflation, retrograde systemic perfusion was maintained via the femoral artery distal to the origin of the MAPCAs. A left atrial ventricular catheter was inserted. Myocardial protection was achieved using intermittent cold antegrade blood and retrograde cardioplegia.
Fig. 4
The fluoroscopy shows that the inflated intra-aortic balloon (arrow) was placed at the origin of the MAPCAs located in the descending aorta
Fig. 5
Transesophageal echocardiography revealed the MAPCA (arrow) originating from the descending aorta. The inflated intra-aortic balloon catheter (arrowhead) blocked the pulmonary blood flow through the MAPCA. Ao, aorta
A large VSD was directly observed under the right coronary cusp. In addition, vegetation was attached to the commissure between the noncoronary and right coronary cusp. During cardiac arrest, the patient’s aortic valve was replaced with a bioprosthetic valve (Inspiris®; Edwards Lifesciences Corporation). During CPB weaning, dobutamine infusion (2.0 µg/kg/min) was initiated to support single ventricle contraction. Balloon catheters were deflated and removed before CPB weaning, which was easily achieved. After weaning, SpO2 was maintained between 80 and 85%, similar to the preoperative value, and targeted a hemoglobin concentration of 15 mg/dL via red blood cell transfusion. Aortic cross-clamping, CPB, surgery, and anesthesia were performed for 115, 191, 520, and 631 min, respectively. The estimated blood loss and urine output were 4341 and 1400 mL, respectively. Overall, 2200 mL crystalloid, 1120 mL packed red blood cells, 960 mL fresh frozen plasma, 400 mL platelet concentrate, and 180 mL cryoprecipitate were administered.
After surgery, the patient was transferred to the intensive care unit with ventilator support under propofol sedation. The patient remained ventilated overnight and was extubated the following day. Four weeks later, the patient was discharged from the hospital without complications. Upon discharge, the oxygen saturation was 79% under oxygen administration (2 L/min via a nasal cannula).
留言 (0)