
記住我






Radiographically, os odontoideum is described as an independent ossicle located posteriorly to the hypertrophic anterior atlas arch, featuring cortical margins, distinct from a hypoplastic dens (1). The anterior arch of the atlas appears enlarged, accompanied by the presence of a small posterior arch. This differs from a recent odontoid fracture. There are two varieties of os odontoideum: the first, termed orthotopic, is positioned behind the anterior arch of the atlas in the normal location where the odontoid process would be (2). The second variety involves cranial migration of the os odontoideum, moving in conjunction with the clivus, and is termed dystopic. The gap beneath the os odontoideum can lead to the incompetence of the cruciate ligament and subsequent craniocervical instability. Even though the volume of literature on os odontoideum has been expanding, questions about its etiology remain a topic of debate, despite the occurrence of congenital, familial, and associated abnormalities (3–14). Moreover, early childhood trauma at the craniocervical junction is one of the leading causes of the traumatic formation of os odontoideum (3, 4, 9). We have conducted an analysis of a large database focusing on both the congenital and traumatic origins of os odontoideum, including associated abnormalities. A literature review spanning from 1970 to 2022 was conducted to validate our findings. The exploration of embryology and blood supply plays a major role in enhancing our understanding of the issue (15–18).
Methods and materialsThe referral database for craniovertebral junction (CVJ) abnormalities was initiated in 1978 (19). Out of a referral base of 520 cases from 1978 to 2022, surgical management was conducted on 260 patients with os odontoideum(). All inpatient and outpatient records were retrospectively reviewed. The following data and variables were recorded: patient age, sex, age of symptomatic presentation, anatomical classification of the os odontoideum, and associated craniocervical junction and systemic abnormalities. All patients were examined by plain radiography and myelotomography as needed until 1984, and since then, CT and MRI have been employed (2). A history of early childhood craniovertebral junction trauma (less than 6 years) was investigated, which included obtaining initial radiographs from emergency departments from the national referral and subsequent follow-up (9). Associated radiographic and systemic abnormalities were noted, and the abnormal atlas development was followed up.
Prior to 1984, all patients underwent plain cervical spine radiography and pluridirectional tomography in the flexed, extended, and lateral bending positions. This was further supplemented with CT imaging, CT myelography, and, at times, vertebral angiography. After 1984, CT myelography was replaced with MRI in the flexed and extended positions, along with CT angiography. 3D CT imaging of the CVJ has been performed in all patients since 1990. Particular attention has been given to facet joint abnormalities in both the forward review and retrospective analysis (20). This manuscript does not delve into the specifics of surgical management.
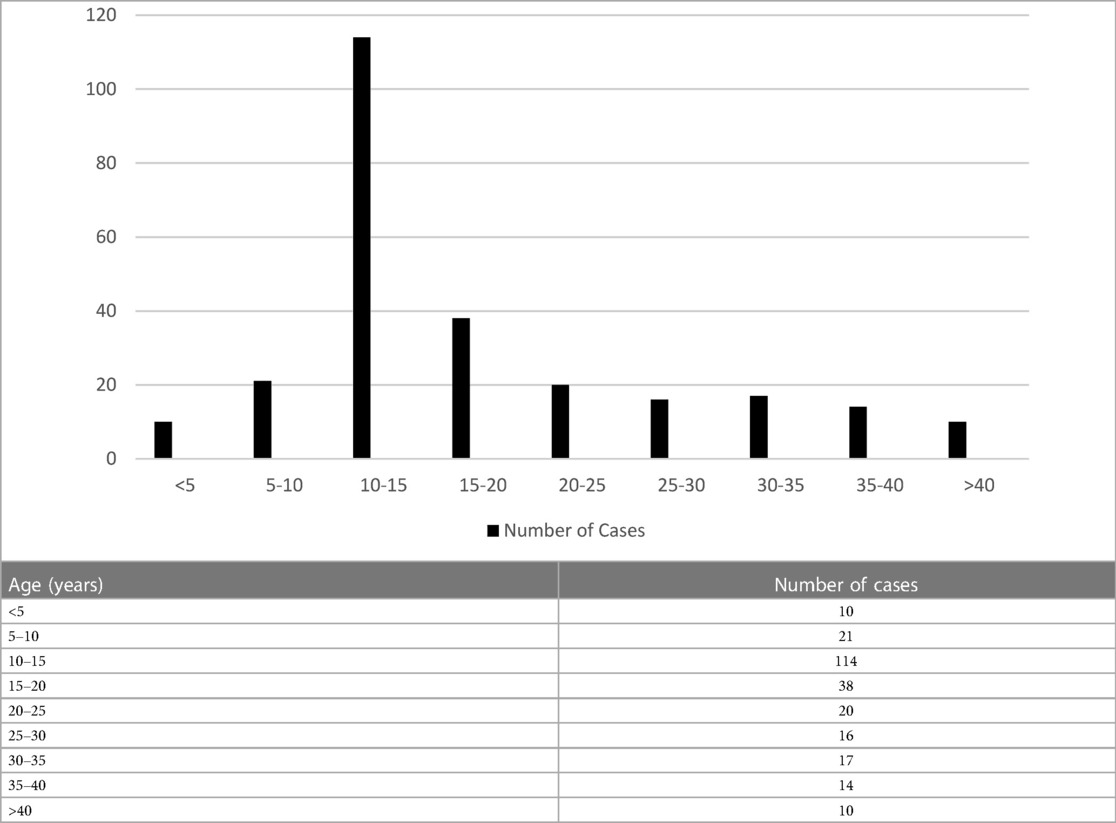
ResultsPatients ranged in age from 4 to 68 years. The age group with the highest number of patients was 10–20 years (Table 1). The youngest symptomatic patient in our study was 4 years old, with os odontoideum development. Children with associated congenital abnormalities presented at an earlier stage (Table 2), although they might have become symptomatic a few years prior. There were 176 males and 86 females in the study.
Table 1. Age at presentation.
Table 2. Associated conditions with os odontoideum (260 patients).
Radiographic findingsApplying a radiographic classification of os odontoideum, the authors identified 24 cases of orthotopic os odontoideum and 236 cases of dystopic os odontoideum. Out of 260 patients, 94 (36%) had associated abnormalities, with 73 exhibiting syndromic abnormalities and 21 having Chiari I malformation. In this congenital variety, a combination of segmentation failure and Chiari abnormality was observed. The associated abnormalities were evidently more prevalent in the pediatric cohort than in adults.
Within the large database of 520 patients, 64 were incidentally identified as having os odontoideum but did not receive initial treatment. Of the 64 patients, 28 exhibited later instability, with a mean of 4 years after diagnosis; among these, 8 were children.
We were unable to identify any variables, such as osseous abnormalities at the atlantoaxial facet joints, that could prevent reduction (20). However, this observation could reflect the characteristics of the patient population.
Early in the series, we encountered two sets of twins with a family history of spondyloepiphyseal dysplasia, both presenting with an unstable os odontoideum (likely ossiculum terminale). Of interest to note is that four children who had previously undergone craniofacial reconstruction for craniofacial dysostosis later showed reducible dystopic os odontoideum.
A history of early childhood craniocervical junction trauma (less than 6 years of age) was investigated, which included obtaining initial radiographs from emergency departments from the national referral and subsequent follow-up. Of the 260 patients, 156 had a previous history of early childhood trauma. We obtained cervical spine documentation of a normal odontoid process at the initial injury in 54 of the 156 patients who subsequently developed os odontoideum. Recently, two patients were documented with craniocervical ligamentous injuries on MRI. Attention was paid to the development of the anterior atlas arch, especially focusing on the anterior tubercle with hypertrophy in post-traumatic cases including gradual shrinkage of the posterior atlas arch. This is further reviewed in the Discussion section of this manuscript. It is related to both the blood supply and embryology.
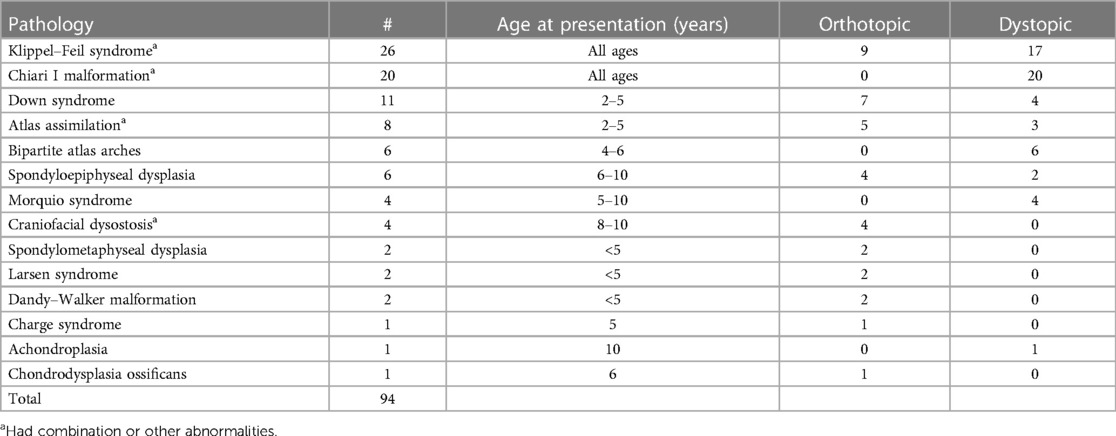
Illustrative cases Case 1In 1989, this 4.5-year-old girl presented with weakness in the arms, numbness in the hands, and a peculiar gait. She had a dystopic os odontoideum with abnormal motion dynamics. The anterior and posterior arches of the atlas appeared to be of normal caliber, but forward motion of the posterior atlas arch in flexion was observed, leading to compression at the cervicomedullary junction, as seen in both pluridirectional tomography and flexion MRI scans (Figure 1A). This was corrected in extension (Figure 1B). She underwent intraoperative crown halo traction and a dorsal occipitocervical fusion procedure using a rib graft. This demonstrates the normal thickness of the anterior and posterior atlas arches, both of congenital origin, accompanied by abnormal motion dynamics.
Figure 1. (A) Composite of midline pluridirectional CVJ tomogram (L) and midsagittal T2-W CVJ MRI in flexion (R). The posterior C1 arch moves forward, and the os odontoideum is seen anteriorly. (B) Same patient as in (A): extension studies.
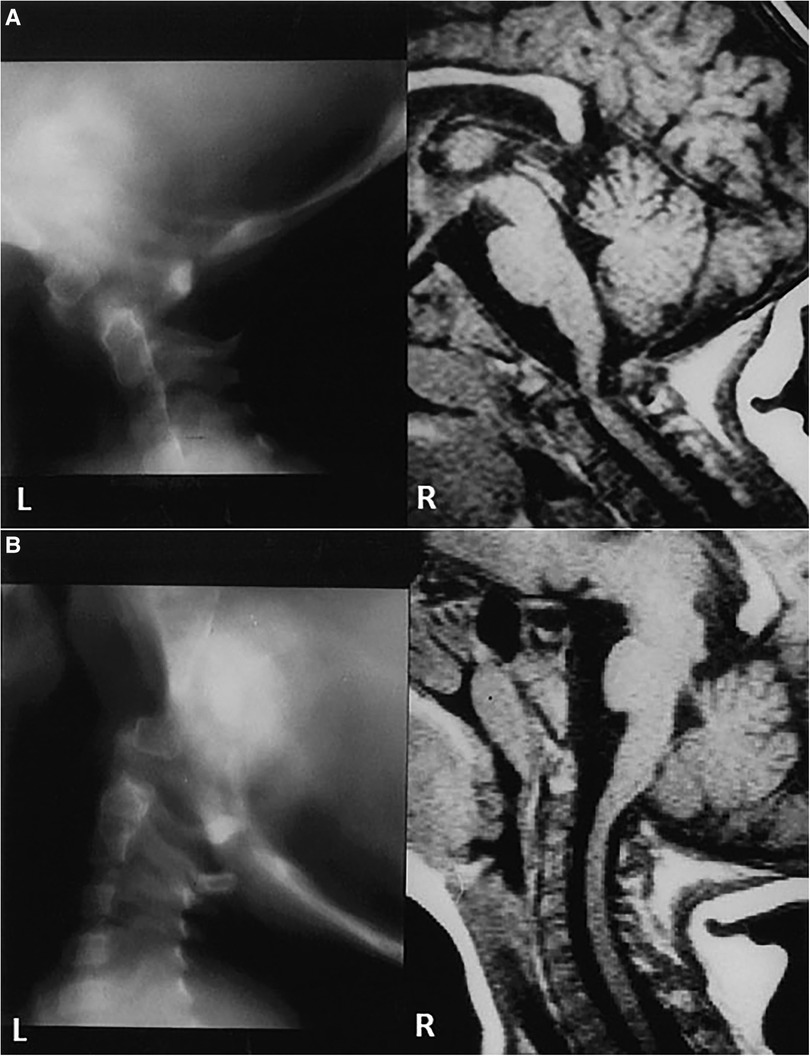
Case 2In 2001, a 6-year-old girl presented with short stature and progressive quadriparesis. A combination of MRI and CT revealed a dislocation at the C1–C2 level, along with os odontoideum and a cruciate ligament over the C2 vertebral body (as indicated by an arrow and confirmed during transoral surgery). There was an hourglass compression of the cervicomedullary junction (Figure 2A). The CT scan demonstrated bifid anterior and posterior arches of C1, with the os odontoideum occupying the space of the diastatic anterior arch of C1 (Figures 2B,C). She underwent an anterior transoral resection of the os odontoideum and the superior aspect of the axis body. She also had a C1 laminectomy with dorsal occiput–C3 fusion using a rib graft (Figure 2D). She achieved a complete neurological recovery.
Figure 2. (A) Midsagittal T1-W MRI of CVJ in a 6-year-old child. Note the cervicomedullary compression by the superior C2 and the dorsal C1 arch. There is an os odontoideum. The arrow demonstrates the cruciate ligament. (B) 2D CT of CVJ of the patient in (A). (C) Axial CT at C1. The anterior arch of C1 is bifid with the os odontoideum in the bipartite space. (D) Lateral cervical radiographs obtained 11 years later. Note the normal alignment and dorsal occipitocervical fusion.
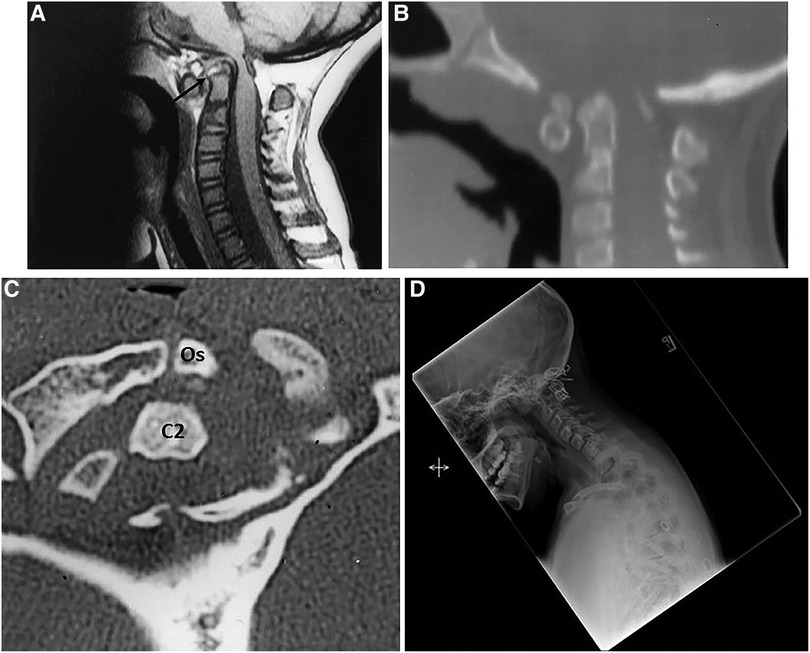
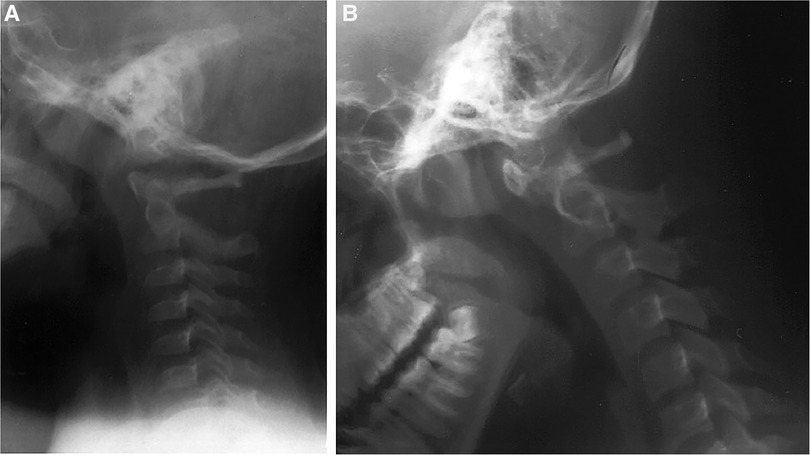
Case 3In 1986, a 4-year-old girl was involved in a motor vehicle accident. The lateral cervical spine radiographs from a local emergency department admission showed an intact odontoid process with widening of the posterior atlantoaxial space and straightening of the cervical spine (Figure 3A). She did well. At the age of 14 years, she presented to us with significant neck pain and paresthesias in her hands. Cervical spine radiographs demonstrated a dystopic os odontoideum (Figure 3B). She underwent a dorsal occipitocervical fusion. This demonstrates a post-traumatic development of os odontoideum. The anterior atlas arch and the anterior tubercle are hypertrophied, while the posterior arch is small and atrophic.
Figure 3. (A) Lateral cervical spine radiograph after motor vehicle accident of a 4-year-old girl, in 1986. Note the widening of C1–C2 interspinous space and the intact odontoid process. (B) Lateral cervical spine X-ray obtained 10 years later [patient in (A)]. There is a C1–C2 dislocation and os odontoideum.
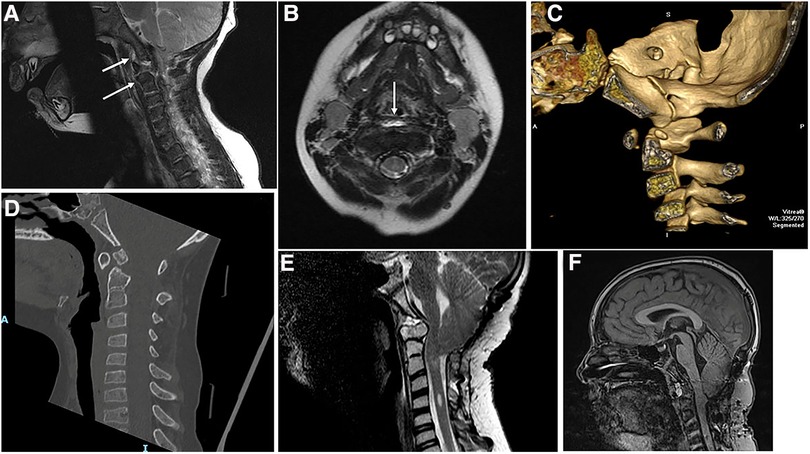
Case 4In 2006, an 18-month-old boy was referred to our facility after falling out of a crib; due to an inability to sit and poor hand movement. He exhibited ecchymosis on his forehead, prompting immediate magnetic resonance imaging with a cervical collar for stabilization. The cervicomedullary junction was enlarged, and there was 8-mm tonsillar herniation, consistent with Chiari I abnormality (Figures 4A,B). On T2-W MRI, there was an area of linear brightness, indicating elevation of the anterior longitudinal ligament in front of C1, C2, and C3 vertebral bodies. A small odontoid process was identified (Figures 4A,B). The assessment suggested craniocervical ligamentous injury, cervicomedullary contusion, and Chiari I abnormality. Significant neurological improvement was observed with the administration of dexamethasone and the use of a cervical brace. Lateral cervical spine radiographs at 2 months showed incomplete development of the anterior and posterior arches of the atlas with normal alignment. Repeat MRI showed soft tissue crowning of the odontoid process and cerebellar tonsillar ectopia. The prevertebral swelling had receded. We investigated the alar and cruciate ligaments, as well as the tectorial membrane, and found them to be intact. A year following his injury, a CT scan of the neck showed irregular ossification of the axis body, a hypoplastic dens, and a small odontoid process (Figure 4C). Seven years later, at age 9, a lateral cervical spine radiograph was performed elsewhere after a school altercation, revealing a dystopic os odontoideum. He subsequently presented to us again with complaints of headaches, difficulty swallowing, bladder incontinence, numbness in his hands, and a tendency to drop objects (Figure 4D). Magnetic resonance imaging showed a Chiari malformation, with the tonsils descending to 20 mm below the plane of the foramen magnum. Gross atlantoaxial instability was observed on cervical dynamic radiographs. He underwent a posterior fossa procedure for Chiari I abnormality and dorsal occipitocervical fusion (Figure 4E). He later presented with progressive Lhermitte's phenomenon and achieved full recovery following transoral decompression of the cervicomedullary junction (Figure 4F). A bony spicule from the posterior surface of the os odontoideum had penetrated the dura.
Figure 4. (A) Midsagittal T2-W MRI of CVJ of an 18-month-old boy. There is a prevertebral bright signal in front of C1–C2 vertebral bodies, (arrows) Chiari I abnormality, and a widened cervicomedullary junction. (B) Axial T2-W MRI through C1of the same patient as in (A). Note the prevertebral signal abnormality (arrow). (C) 3D CT of CVJ in midsagittal reconstruction made at the age of 2.5 years. A small ossicle is seen above the odontoid. (D) 2D CT of CVJ reveals an os odontoideum at the age of 10 years. (E) Midsagittal T2-W MRI of CVJ after posterior fossa decompression and dorsal occipitocervical fusion. There is ventral compression by the os odontoideum. (F) Midsagittal T2-W MRI of CVJ done after transoral resection of the os odontoideum.
This is MRI documentation of craniocervical ligamentous injury with sequential formation of os odontoideum.
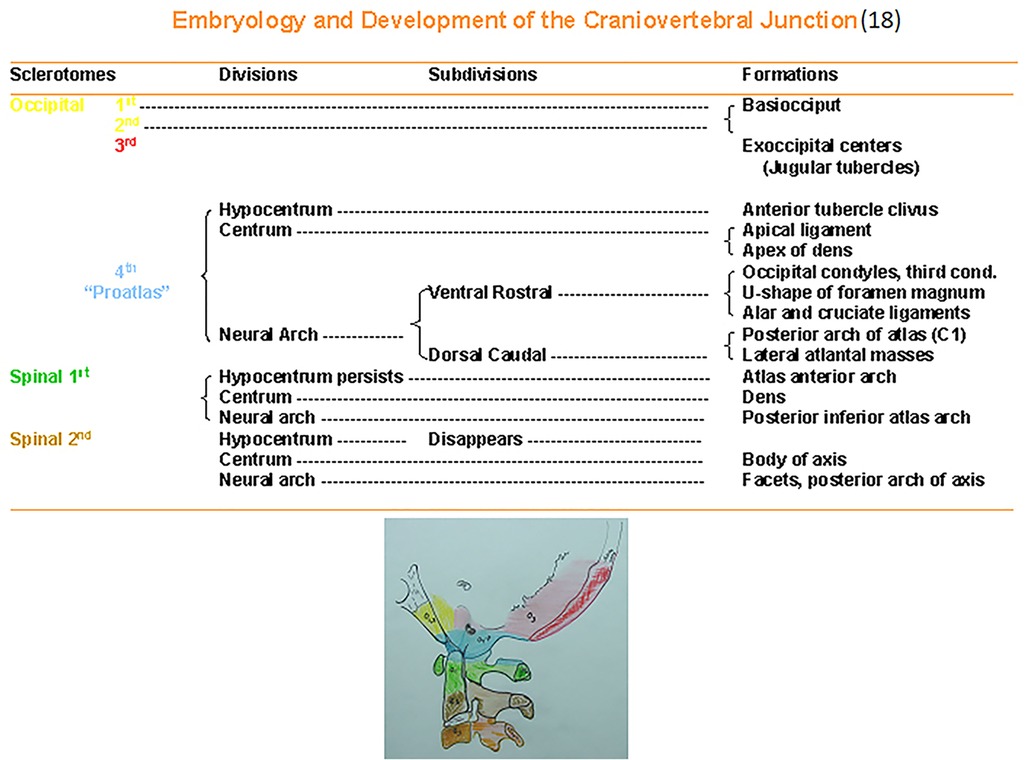
Discussion Embryology and vascular supply of the bony architecture of the craniovertebral junctionThe relevant embryology is summarized to provide an understanding of the etiology of os odontoideum (2, 15, 18). At 4 weeks gestation, there are 42 somites, of which four are occipital and eight are cervical. Each somite divides into an outer dermatome, an inner myotome, and a medial sclerotome. The sclerotomes are located ventromedially and will form the vertebral bodies. The first four sclerotomes will fuse to form the occipital bone and the posterior portions of the foramen magnum. There are simultaneous vascularization and differentiation of the ganglia and vascular tissues. The fourth sclerotome serves as the foundation for understanding the craniocervical junction and is termed proatlas.
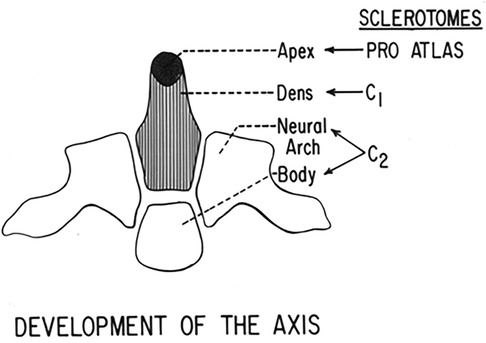
Figure 5 identifies the embryology and development of the craniocervical junction and provides ease of reference. The proatlas divides into a ventral rostral segment and a corresponding dorsal caudal portion. This latter forms the posterior arch and the lateral masses of the atlas. The ventral component of the proatlas forms the anterior U-shaped margin of the foramen magnum and the occipital condyles. A portion of the ventral component of the proatlas detaches and integrates with the pleural centrum of the atlas vertebra, which develops as a dens. The core of the atlas centrum is metamorphosized into the apical ligament of the dens. The atlas, the check ligaments, and the transverse ligament of the atlas are derived from the proatlas as unossified tissue. The dens component of the odontoid process actually represents the atlas centrum. At birth, the odontoid is separated from the body of the axis by a cartilaginous band, representing a vestigial disc referred to as neurocentral synchondrosis (Figure 6). This lies below the level of the superior articular facets of the axis and does not represent the anatomical basis of the dens. Neurocentral synchondrosis is present in nearly all children by the age of 3 years and is absent in most by the age of 6–8 years. At birth, a recognizable odontoid process should be which has not yet fused to the base of the axis. The tip of the odontoid process is not ossified and is represented by a separate ossification center (from proatlas), which is usually seen at age 3 years and fuses with the body of the dens. A second spinal sclerotome contributes to the caudal portion of the axis body and the arches.
Figure 5. Embryology and development of the craniovertebral junction (18).
Figure 6. Development of the axis vertebra.
The axis vertebra is biomechanically adapted to encourage motion while preserving stability (21). The complex anatomy of the craniovertebral articulation provides stability reinforced by the ligaments and membranes that contribute to the stability of the occipital–atlantoaxial complex.
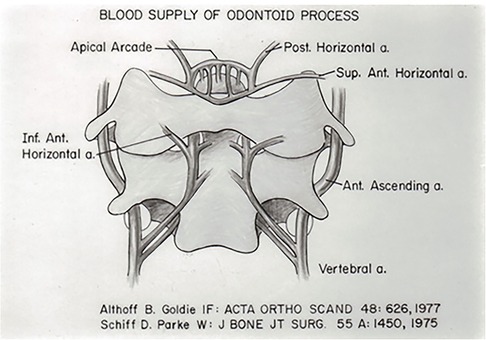
The blood supply to the odontoid process originates from two sources (16, 17, 22). The vertebral arteries supply anterior and posterior ascending arteries that course ventral and dorsal to the body of the axis and the odontoid and anastomose in an apical arcade in the region of the alar ligament (Figure 7). These vessels supply the small perforating branches of the body of the axis and the odontoid process. In addition, the anterior ascending arteries and the apical arcade receive contributions from the carotid artery through the base of the skull and the alar ligament. Thus, the organization of the blood supply has an embryologic origin (16, 22).
Figure 7. Blood supply of the odontoid process.
According to proponents of the embryological formation for the os odontoideum, it is purportedly a result of the failure of fusion between the dens and the axis body (23). If this were the case, the gap between the os odontoideum and the axis should be located below the level of the superior axis facets. However, this has never been demonstrated. In addition, in all patients with the presence of an os odontoideum, a neurocentral synchondrosis is almost always visible. However, os odontoideum is associated with numerous conditions such as segmentation failure with Klippel–Feil syndrome, atlas assimilation, Down syndrome, Morquio syndrome, and skeletal dysplasias (Table 2) (9, 11, 15, 16, 24, 26–30). In our series, there were two sets of twins with spondyloepiphyseal dysplasia. In a study conducted at the Children's Hospital of Philadelphia between 1991 and 2004 on 16 cases of os odontoideum, it was found that half of the patients (eight) reported a history of trauma. Among the remaining eight cases, six exhibited associated congenital abnormalities of the cervical spine and three were diagnosed with genetic syndromes (31). It is also possible that the os odontoideum results from the failure of proper caudal migration of the odontoid process during development (25). An alternative hypothesis proposes the failure of segmentation of the dens from the anterior arch of the atlas, resulting in the “jigsaw sign” (32). Analysis of our database comprising 260 patients revealed that 94 had associated congenital bony abnormalities (36%), with 73 exhibiting syndromic abnormalities and 21 showing Chiari I malformation. The congenital variety showed early presentation as per our population-based study. In addition, it is important to recognize that in congenital syndromic abnormalities, the complication rate, as described in the literature, was 40%, in contrast to 15% in non-syndromic cases (33, 34). Numerous case reports document the presence of os odontoideum in families, suggesting a hereditary nature, and in twins (10–12, 14, 26, 31, 33, 35–37). In the congenital variety, we have recognized that the anterior arch is not hypertrophied, nor is there atrophy of the posterior arch of the atlas. This could be because of early presentation as opposed to those with traumatic origin.
During development, the odontoid process has an apical component from the proatlas (fourth occipital sclerotome), a contribution from the centrum of C1 to form the body of the odontoid process, and involvement of the C2 sclerotome that forms the base (15, 18). Between each of these components is the upper neurocentral synchondrosis, with the lower forming the lowest synchondrosis, also known as the neurodental synchondrosis. It has been suggested that trauma occurring in early childhood between the upper and lower synchondrosis can lead to either a fracture or stress, affecting the vascular supply to the odontoid process (4, 9, 25). The apex would remain viable, and with contracture of the apical and alar ligaments, this pulls the odontoid segment away from the C2 body, resulting in the formation of os odontoideum. This also explains the hypertrophy of the anterior arch of the atlas and the atrophy of the posterior atlas arch. In our series of 260 patients who underwent surgical treatment, 156 had a history of early childhood trauma and 54 had documentation of a normal odontoid process at the initial injury, for which we were able to obtain these images from the emergency departments around the country where these children were first encountered. In these 54 cases, the subsequent development of os odontoideum was documented, and patients were referred due to neck pain, neurological deficit, and acute worsening with trauma. In none of these post-traumatic groups did we observe bony abnormalities, which seemed to have been reserved for the congenital variety.
It is only recently that patients with initial trauma have undergone CT or MRI scanning at the initial injury.
ConclusionsThe etiology of os odontoideum is multifactorial. There does exist a congenital variety in which associated bony and syndromic abnormalities are present. There is a question of whether the congenital variety represents an ossiculum terminale persistens, implying changes in the proatlas segment of the odontoid origin. These individuals present much earlier than the post-traumatic variety. Analysis of a large database contributes to a better understanding of the etiology.
Data availability statementThe original contributions presented in the study are included in the article/supplementary materials, further inquiries can be directed to Arnold Menezes arnold-menezes@uiowa.edu.
Author contributionsAM: Conceptualization, Data curation, Formal Analysis, Investigation, Methodology, Project administration, Supervision, Validation, Writing – original draft, Writing – review & editing.
FundingThe author declares that no financial support was received for the research, authorship, and/or publication of this article.
AcknowledgmentsThe author acknowledges Mary Jo Piper for her assistance in formatting the paper and managing the database.
Conflict of interestThe author declares that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Publisher's noteAll claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
References3. Fielding JW, Griffin PP. Os odontoideum: an acquired lesion. J Bone Joint Surg Am. (1974) 56A(1):187–90. doi: 10.2106/00004623-197456010-00023
CrossRef Full Text | Google Scholar
4. Fielding JW, Hensinger RN, Hawkins RJ. Os odontoideum. J Bone Joint Surg Am. (1980) 62A(3):376–83. doi: 10.2106/00004623-198062030-00007
CrossRef Full Text | Google Scholar
5. Hadley MN, Walters BC, Grabb PA, Oyesiku NM, Przybylski GJ, Resnick DK, et al. Guidelines for management of acute cervical spinal injuries. Introduction. Neurosurgery. (2002) 50(3Suppl):S148–55. doi: 10.1097/00006123-200203001-00003
PubMed Abstract | CrossRef Full Text | Google Scholar
6. Hammerstein J, Russo S, Easton K. Atlantoaxial dislocation in a child secondary to a displaced chondrum terminale. A case report. J Bone Joint Surg Am. (2007) 89:413–7. doi: 10.2106/JBJS.E.00595
PubMed Abstract | CrossRef Full Text | Google Scholar
10. Sherk HH, Dawoud S. Congenital os odontoideum with Klippel-Feil anomaly and fatal atlanto-axial instability. Report of a case. Spine. (1981) 6(1):42–5. doi: 10.1097/00007632-198101000-00007
PubMed Abstract | CrossRef Full Text | Google Scholar
11. Went C, Wang LM, Wang WD, Tan HY. Bipartite atlas with os odontoideum and synovial cyst. Case report and review literature. Spine. (2010) 35:E568–75. doi: 10.1097/BRS.0b013e3181b9c9c0
PubMed Abstract | CrossRef Full Text | Google Scholar
13. McHugh BJ, Grant RA, Zupon AB, DiLuna ML. Congenital os odontoideum arising from the secondary ossification center without prior fracture. J Neurosurg Spine. (2012) 17:594–7. doi: 10.3171/2012.9.SPINE12824
PubMed Abstract | CrossRef Full Text | Google Scholar
19. Menezes AH. Congenital and acquired abnormalities of the craniovertebral junction. In: Youmans JR, editor. Neurological surgery. Philadelphia: WB Saunders (1995). p. 1035–89.
20. Dlouhy BJ, Policeni BA, Menezes AH. Reduction of atlantoaxial dislocation prevented by pathological position of the transverse ligament in fixed, irreducible os odontoideum: operative illustrations and radiographic correlates in 41 patients. J Neurosurg Spine. (2017) 27:20–8. doi: 10.3171/2016.11.SPINE16733
PubMed Abstract | CrossRef Full Text | Google Scholar
21. Menezes AH, Traynelis VC. Anatomy and biomechanics of normal craniovertebral junction (a) and biomechanics of stabilization (b). Childs Nerv Syst. (2008) 24(10):1091–100. doi: 10.1007/s00381-008-0606-8
PubMed Abstract | CrossRef Full Text | Google Scholar
22. Schiff DC, Parke WW. The arterial supply of the odontoid process. J Bone Joint Surg Am. (1973) 55A:1450–6. doi: 10.2106/00004623-197355070-00012
CrossRef Full Text | Google Scholar
24. Zhao D, Wang S, Passias PG, Wang C. Craniocervical instability in the setting of os odontoideum: assessment of cause, presentation, and surgical outcomes in a series of 279 cases. Neurosurgery. (2015) 76:514–21. doi: 10.1227/NEU.0000000000000668
PubMed Abstract | CrossRef Full Text | Google Scholar
25. Zygourakis CC, Cahill KS, Proctor MR. Delayed development of os odontoideum after traumatic cervical injury: support for a vascular etiology. J Neurosurg Pediatrics. (2011) 7:201–4. doi: 10.3171/2010.11.PEDS10289
CrossRef Full Text | Google Scholar
26. Goel A, Patil A, Shah A, Dandpat S, Rai S, Ranjan S. Os odontoideum: analysis of 190 surgically treated cases. World Neurosurg. (2020) 134:e512–23. doi: 10.1016/j.wneu.2019.10.107
PubMed Abstract | CrossRef Full Text | Google Scholar
27. Hericord O, Bosschaert P, Menten R, Dembour G. Misleading appearance of atlantoaxial diastasis in down syndrome: os odontoideum. JBR-BTR. (2009) 92:261.19999333
PubMed Abstract | Google Scholar
28. Taggard DA, Menezes AH, Ryken TC. Treatment of down syndrome-associated craniovertebral junction abnormalities. J Neurosurg. (2000) 93(2 Suppl):205–13. doi: 10.3171/spi.2000.93.2.0205
PubMed Abstract | CrossRef Full Text | Google Scholar
29. Arvin B, Fournier-Gosselin MP, Fehlings MG. Os odontoideum: etiology and surgical management. Neurosurgery. (2010) 66:A22–31. doi: 10.1227/01.NEU.0000366113.15248.07
CrossRef Full Text | Google Scholar
31. Sankar WN, Wills BPD, Dormans JP, Drummond DS. Os odontoideum revisited: the case for a multifactorial etiology. Spine. (2006) 31:979–84. doi: 10.1097/01.brs.0000214935.70868.1c
PubMed Abstract | CrossRef Full Text | Google Scholar
32. Fagan AB, Askin GN, Earwaker JW. The jigsaw sign. A reliable indicator of congenital aetiology in os odontoideum. Eur Spine J. (2004) 13:295–300. doi: 10.1007/s00586-004-0732-2
PubMed Abstract | CrossRef Full Text | Google Scholar
33. Helenius IJ, Bauer JM, Verhofste B, Sponseller PD, Krengel WF, Hedequist D, et al. Os odontoideum in children. Treatment outcomes and neurological risk factors. J Bone Joint Surg Am. (2019) 101A:1750–60. doi: 10.2106/JBJS.19.00314
CrossRef Full Text | Google Scholar
34. Saarinen AJ, Bauer JM, Verhofste B, Sponseller PD, Krengel WF, Hedequist D, et al. Results of conservative and surgical management in children with idiopathic and nonidiopathic os odontoideum. World Neurosurg. (2021) 147:e324–33. doi: 10.1016/j.wneu.2020.12.043
留言 (0)